













 5 / 37
5 / 37

Page 31
Volume 09
Otolaryngology: Open Access
ISSN: 2161-119X
ENT 2019
Craniofacial Surgery 2019
August 15-17, 2019
JOINT EVENT
conferenceseries
.com
August 15-17, 2019 Rome, Italy
&
3
rd
International Conference on
Craniofacial Surgery
4
th
European Otolaryngology-ENT Surgery Conference
Tubed supraclavicular flap reconstruction of total pharyngectomy defects for carcinoma hypopharynx
Sashikanth Jonnalagadda
Fellowship in Head and Neck surgery
Consultant and Head, Department of Head and Neck Oncology and ENT
American Oncology Institute, India
C
arcinoma of Hypopharynx is challenging to manage because of the delayed presentation resulting in advanced
nature of the disease at the time of diagnosis . In advanced cases with T3 and T4 tumors usually require total
laryngectomy and total pharyngectomy and this results a reconstruction challenge because of the circumferential
nature of the defect. Traditional reconstruction has been through gastric pull but recently tubed radial forearm free
flap is increasing being employed in such reconstructions. Gastric pull has significant disadvantages because of the
increased morbidity, need of second surgeon and prolonged hospital stay. Free Flap need micro vascular expertise
not widely available and some postradiated patients are extremely challenging because of the recipient vessel status.
Hence, we started using tubed supraclavicular flap in the reconstruction of total pharyngectomy defects and here
we present our experience including the challenges encountered in 7 patients so far. 4/7 patients had post cricoid
carcinoma and 3/7 had pyriform sinus carcinoma with extension to postcricoid region. 5/7 had salvage surgery
following recurrence with Chemo-radiation. The indications for this type of reconstruction in our study included
only circumferential defects with lower of the defect being above the thoracic inlet. Average length of defect was
around 7 cms with range being 5.5 to 9 cm. Wide supraclavicular flap was harvested over the deltoid area usually
from the side of the defect and tubed over a Montgomery salivary bypass tube before suturing over the defect.
Complications included Pharyngo cutaneous fistula in 4 patients out of which 3 resolved with conservative treatment.
We conclude that tubed supraclavicular flap is an easy less morbid alterative that should receive more attention in the
reconstruction of circumferential defects which lie above the thoracic inlet.
Biography
Dr. Sashikanth Jonnalagadda has completed M.S (ENT) from Bangalore Medical College in 2005. Later he received Clinical Fellowship training in Rhinology at
Lahey clinic, Boston, Massachusetts, (USA) and Clinical fellowship in Head and Neck surgery from Southern Illinois University, Springfield, Illinois (USA). Since
2012 he is working as Consultant and Head, Department of Head and Neck Oncology and ENT in American Oncology Institute, Hyderabad, India. His interests
include Thyroid and parathyroid surgeries, Reconstruction in head and neck and endoscopic skull base surgery.
drsashikanth@americanoncology.comSashikanth Jonnalagadda, Otolaryngol (Sunnyvale) 2019, Volume 09
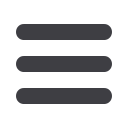
Patient at 5 Month Post -Op
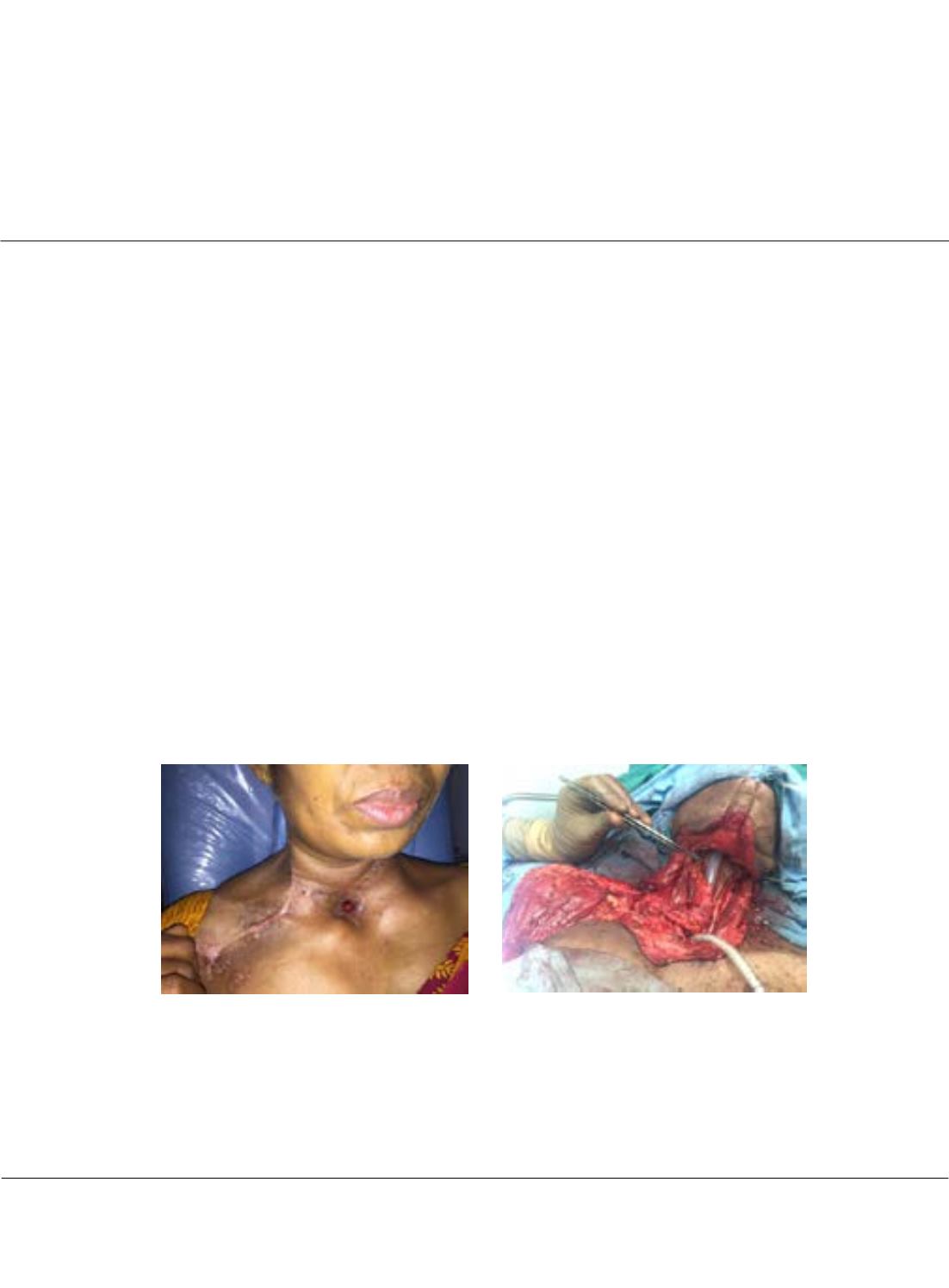
Supra Clavicular flap tubed over a Montgomery
tube-Intra-OP