 Spanish
Spanish  Chinese
Chinese  Russian
Russian  German
German  French
French  Japanese
Japanese  Portuguese
Portuguese  Hindi
Hindi Our Group organises 3000+ Global Conferenceseries Events every year across USA, Europe & Asia with support from 1000 more scientific Societies and Publishes 700+ Open Access Journals which contains over 50000 eminent personalities, reputed scientists as editorial board members.
Open Access Journals gaining more Readers and Citations
700 Journals and 15,000,000 Readers Each Journal is getting 25,000+ Readers
Recommended Conferences
42nd Global Conference on Nursing Care & Patient Safety
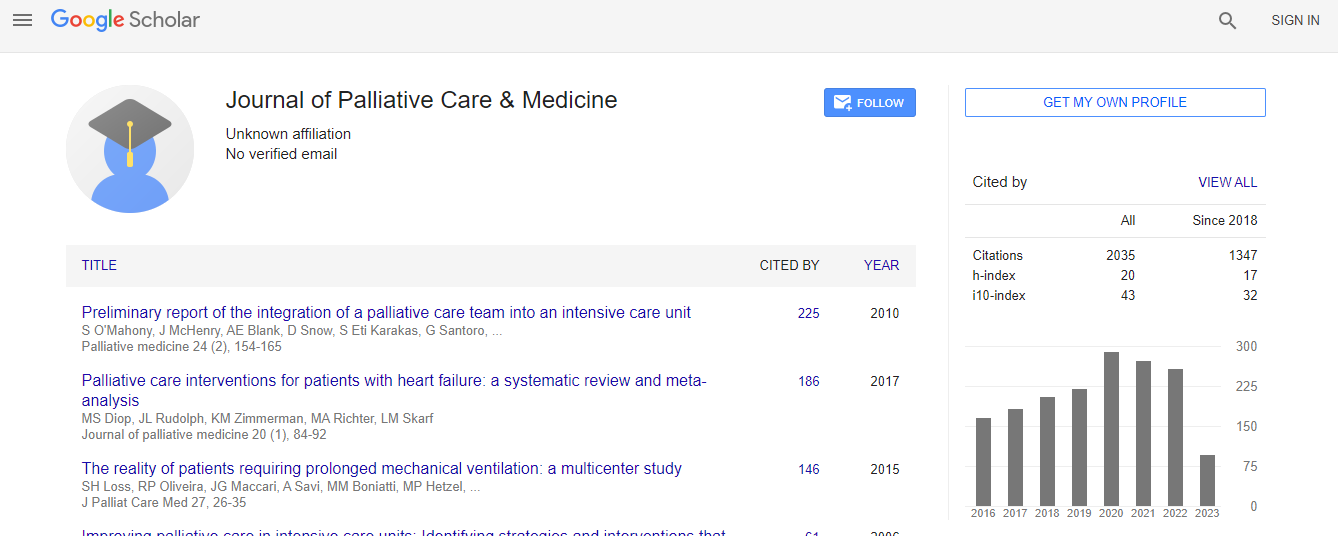
Toronto, CanadaGoogle Scholar citation report
Citations : 2035
Journal of Palliative Care & Medicine received 2035 citations as per Google Scholar report
Journal of Palliative Care & Medicine peer review process verified at publons

Indexed In
- Index Copernicus
- Google Scholar
- Open J Gate
- Genamics JournalSeek
- China National Knowledge Infrastructure (CNKI)
- Electronic Journals Library
- RefSeek
- Hamdard University
- EBSCO A-Z
- OCLC- WorldCat
- Virtual Library of Biology (vifabio)
- Publons
- Geneva Foundation for Medical Education and Research
- Euro Pub
- ICMJE
Useful Links
Recommended Journals
Related Subjects
Share This Page
Tropical Spastic Paraparesis and End of Life Care
3rd International Conference on Palliative Care & Hospice Nursing
Hala Sheikh-Mohamed, Faisal Rahim, Mery Lossada, Sergey Kachur and Justin Reed
University of Central Florida, USA
ScientificTracks Abstracts: J Palliat Care Med
Abstract
The benefits of shared decision making in medical management are well established, but implementing its principles is often a difficult task. It involves extended conversations with patients, with obstacles including cultural and language barriers. Such barriers can be difficult to overcome, particularly with decisions involving death and end of life care. A 73-year-old Haitian woman with history of spastic hyper-reflexic paraparesis, recurrent urinary tract infections (UTI) and chronic hyperkalemia presented to the emergency room with her daughter for back pain and dysuria, following a year-long history of multiple hospitalizations for pain and UTIs. She had worsening confusion, poor appetite, and occasional upper extremity trembling. Examination revealed a demented patient with abdominal tenderness and 3+ hyper-reflexic paraparesis of the lower extremities. Labs showed leukocytosis and hyperkalemia with a polymicrobial urine culture growing ESBL E. coli and Pseudomonas aeruginosa for which she was started on meropenem. Transtubular potassium gradient indicated renal tubular acidosis as a cause of her hyperkalemia and treatment with fludrocortisone corrected her potassium. Despite almost a week of treatment there was little clinical improvement; the patient was bed-bound and had poor appetite. Given her significant disability, testing for HTLV in the CSF (indicative of tropical spastic paraparesis) was performed, and came back positive. The patient��?s condition and prognosis as well as the family��?s values were discussed throughout, and as the burden of her chronic disease became evident, the consensus was to maintain comfort and request additional care through hospice. Thus, she was referred to hospice for symptom palliation, and she passed away surrounded by family two weeks later. The lack of adequate communication with this patient and her family over several hospitalizations initially resulted in a care plan that was not aligned with the patient��?s values and understanding of her prognosis. Although her urine cultures were repeatedly treated with antibiotics, there was no meaningful recovery and this likely contributed to the development of her multi-drug resistant bacteria. With the current shift toward personalized medicine, it is important to involve a multidisciplinary team that includes the patient, family, and physicians to make collaborative decisions. Such an approach contributes to holistic care and outcomes better aligned with patient values; improved patient quality of life, better family perceptions of the healthcare system and lower potential costs from readmissions.Biography
Hala Sheikh-Mohamed is currently doing her Internal Medicine Residency at the University of Central Florida/HCA consortium and hopes to pursue a fellowship in Hematology-Oncology in the near future. Dr. Sheikh-Mohamed is passionate about the early diagnosis and management of triple negative breast cancer but has unfortunately experienced limited early integration of palliative care services for patients undergoing treatment for these aggressive cancers. Dr. Sheikh-Mohamed hopes to work towards establishing a more standardize incorporation of early palliative care services that will address the early symptom burden, quality of life, and end of life care needs of all medical oncology patients.