 Spanish
Spanish  Chinese
Chinese  Russian
Russian  German
German  French
French  Japanese
Japanese  Portuguese
Portuguese  Hindi
Hindi Our Group organises 3000+ Global Conferenceseries Events every year across USA, Europe & Asia with support from 1000 more scientific Societies and Publishes 700+ Open Access Journals which contains over 50000 eminent personalities, reputed scientists as editorial board members.
Open Access Journals gaining more Readers and Citations
700 Journals and 15,000,000 Readers Each Journal is getting 25,000+ Readers
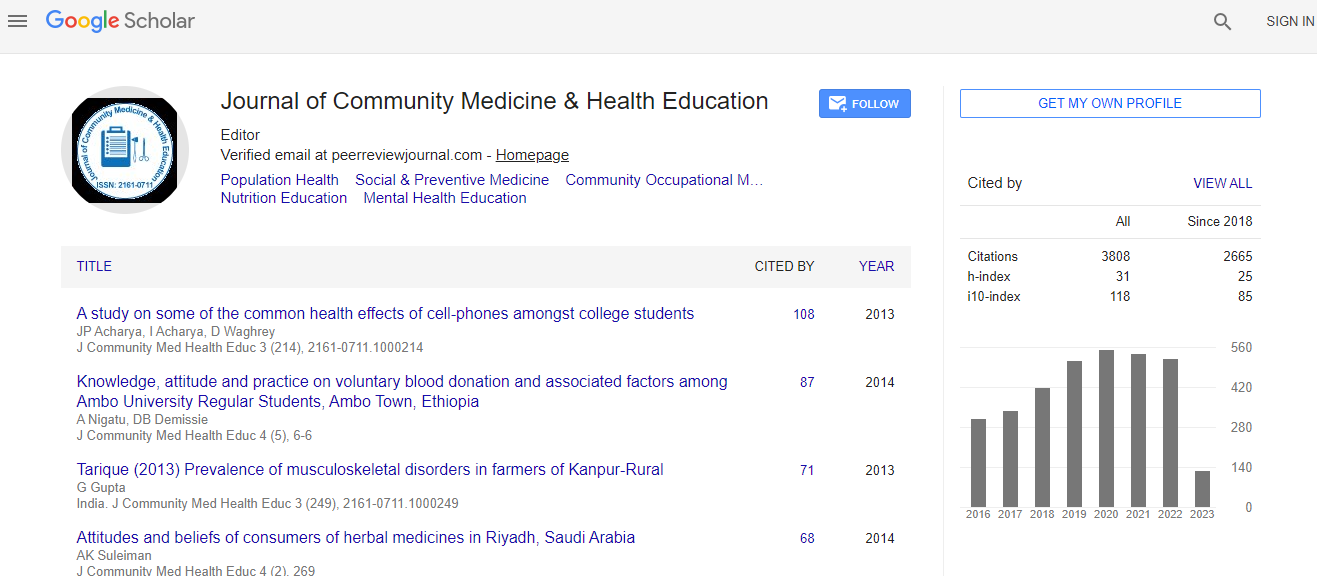
Google Scholar citation report
Citations : 5447
Journal of Community Medicine & Health Education peer review process verified at publons

Indexed In
- Index Copernicus
- Google Scholar
- Sherpa Romeo
- Genamics JournalSeek
- SafetyLit
- RefSeek
- Hamdard University
- EBSCO A-Z
- OCLC- WorldCat
- Publons
- Geneva Foundation for Medical Education and Research
- Euro Pub
- ICMJE
Useful Links
Recommended Journals
Related Subjects
Share This Page
Kyasanur forest disease surveillance system evaluation, Shivamogga, Karnataka and Sindhudurg, Maharashtra, India � 2016-2017
4th World Congress on Public Health, Epidemiology & Nutrition
Ashok Kumar Talyan, Nataraju Seegekote Mariyappa, Pradeep Khasnobis, C S Agarwal, Pavana Murthy, SanketV Kulkarni, Ruchi Jain, Rajesh Yadav, Ekta Saroha, Samir V Sodha, A C Dhariwal and Sujeet Singh
National Centre for Disease Control, India World Health Organization, India Centers for Disease Control and Prevention, India Centers for Disease Control and Prevention, USA
Posters & Accepted Abstracts: J Community Med Health Educ