













 7 / 9
7 / 9

Page 47
Notes:
May 16-17, 2018 | Montreal, Canada
World Congress on
Cardiology and Cardiac Surgery
Journal of Clinical & Experimental Cardiology | Volume: 9
Surgical results of Ebstein’s anomaly based on pathology and techniques
Qingyu Wu
and
Xiaoya Zhang
Tsinghua University, China
Objective
: The objective of this study was to evaluate the outcomes of patients who underwent the different techniques
according to the pathology of Ebstein anomaly (EA).
Methods
: From March 2004 to February 2017, 228 patients (mean age, 19.8±15.4 years; range, 7 months-64 years) with EA
underwent 232 cardiac operations at our hospital. Twenty-nine patients had a prior cardiac procedure before. Among the
patients in first procedures, 92 patients (46.2%) were categorized to Carpentier type C and 63 patients (31.7%) were type D,
7 patients (3.5%) had isolated anterior leaflet downward displacement. Anatomical repair were performed in 179 patients
(Type B, n=35; type C, n=92; Type D, n=29; unclassifiable, n=7; reoperation, n=16), 1½ ventricle repair in 37 (Type D, n=33;
reoperation, n=4), tricuspid valve repair in 3 (Type A, n=2; Type B, n=1), tricuspid valve replacement in 10 (7 reoperations),
and Fontan procedure in 3 (TCPC, n=2; Glenn, n=1). Atrialized right ventricle was presented in 194 cases (168 excised, 6
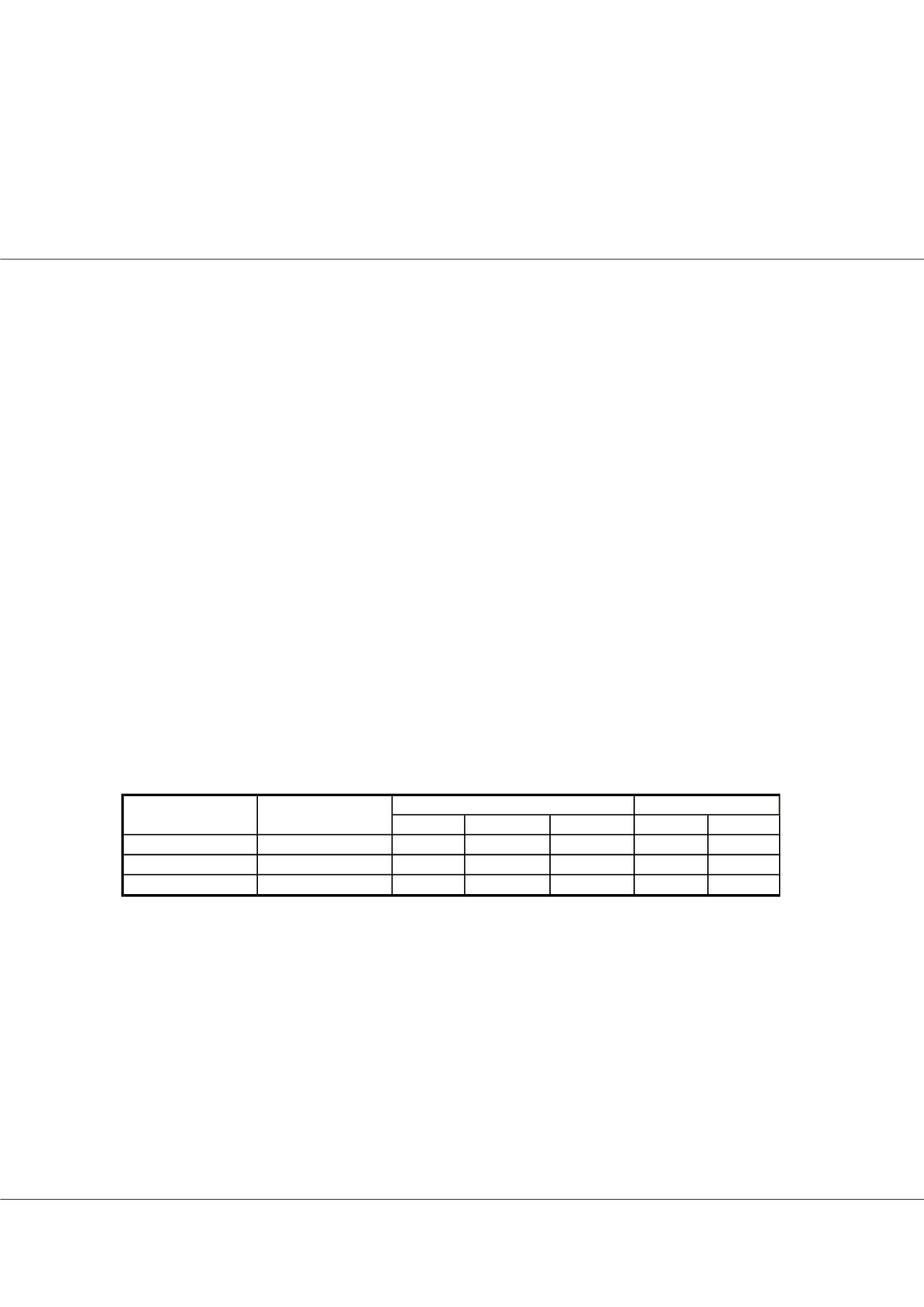
incorporated). The pathology of 199 patients who underwent first procedures at our center described in Table 1.
Results
: The mortality was 1.7% (n=4: anatomical repair, n=3; 1½ ventricle repair, n=1). Among these, 1 pathology type was
Carpentier type C and 3 were type D. 1 A-V block (0.4%) newly occurred. 214 patients were available to follow up. The range
of follow-up duration was 10 months to 13 years (mean, 7.3±3.2 years). Late survival was 99% (2 late deaths) at 10 years. Three
patients received reoperation (reoperation rate, 1.3%; TVR, n=1; 1½ ventricle repair, n=2). Mean New York Heart Association
class improved from 3.5 to 1.1.
Conclusions
: The principle of the techniques is to reconstruct the tricuspid valve and right ventricle anatomically. For most
cases, the anatomical repair was demonstrated with low mortality, less complications and excellent durability at long-term
follow-up. The Carpentier classification cannot categorize all the patients. It is critical to choose applicable surgical techniques
individually according to the pathologic morphology for EA surgical results. If the tricuspid valve is severely hypoplastic, 1½
ventricle repair and valve replacement may be alternative.
Biography
Qingyu Wu has completed his graduation from Sun Yat-sen University of Medical Sciences in 1976, then worked at Fuwai Hospital, completed his MD at Peking
Union Medical College in 1982 and trained at The Prince Charles Hospital in Brisbane, Australia. In 2004, he has moved to The First Hospital of Tsinghua University
to establish a new Heart Center. He has practiced in Pediatric and Adult Cardiovascular Surgery for 42 years and had not only remarkably reduced the mortality of
surgical treatment of coronary disease in China, but also created and improved a variety of surgical procedures in TGA, CABG, Ebstein anomaly, single ventricle,
DORV, TOF and so on. He has published 278 papers and 14 books, won five times the National Science and Technology Progress Awards. He has been invited to
perform operations in other countries for six times.
wuqingyu@mail.tsinghua.edu.cnQingyu Wu et al., J Clin Exp Cardiolog 2018, Volume: 9
DOI: 10.4172/2155-9880-C4-098
Normal Displaced Adherent Normal
Small
Anterior
4
54
137
4
59
129
Posterior
70
17
105
7
5
124
Septal
65
9
113
12
3
131
Tricuspid leaflet
Totally Abasent
Leaflet
position
Leaflet
Size