Case Report Open Access
Unexpected Patch Test Complication in a Professional Ice Hockey Player
Magnus Bruze1, Tomas Eriksson1, Marléne Isaksson1* and Yelverton Tegner21Department of Occupational and Environmental Dermatology, Skåne University Hospital, Lund University, Malmö, Sweden
2Yelverton Tegner, Division of Medical Sciences, Department of Health Sciences, Luleå University of Technology, Luleå, Sweden
- *Corresponding Author:
- Isaksson M
Department of Occupational and Environmental Dermatology
Jan Waldentröms gata 16, level 5, Skåne University Hospital
SE 205 02 Malmö, Sweden
Tel: +46 40 337859
E-mail: marlene.isaksson@med.lu.se
Received date: February 15, 2016; Accepted date: February 26, 2016; Published date: February 29, 2016
Citation: Bruze M, Eriksson T, Isaksson M,Tegner Y (2016) Unexpected Patch Test Complication in a Professional Ice Hockey Player . Occup Med Health Aff 4:229. doi: 10.4172/2329-6879.1000229
Copyright: © 2016 Isaksson M, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Visit for more related articles at Occupational Medicine & Health Affairs
Abstract
In a survey on work-related skin problems in professional ice hockey players one player developed a severe patch test reaction with an unexpected complication. The positive reaction to diethyl thiourea was vesiculo-bullous, oedematous and significantly elevated and a spreading several centimeters outside the test area was noted. Starting less than 24h after the patch test application, itching erythematous, multiforme-like lesions appeared on the extremities. The lesions were interpreted as a manifestation of a systemic allergic contact dermatitis secondary to the patch tested allergen. As systemic corticosteroids are considered as doping, we had to treat him with topical clobetasol propionate. Systemic allergic contact dermatitis seems to be an extremely rare complication after patch testing. It has been reported after testing with some textile disperses dyes but not after testing with diethyl thiourea and is not described as a complication in major textbooks.
Keywords
Systemic contact Dermatitis; Contact allergy; Patch testing; Diethyl thiourea; Erythema Multiforme-like; Neoprene rubber
Abbreviations
DET: Diethyl Thiourea
Introduction
We are currently performing a survey on work-related skin problems in professional ice hockey players in 26 teams in Sweden. The project was approved by the “ethics committee” of the medical faculty, Lund University. The survey is based on questionnaires answered by the players in all teams and patch testing of players in 6 teams. One player developed a severe patch test reaction with an unexpected complication which is reported in this paper.
Case Presentation
The players in one team were patch tested in the sport center after a game on a Friday evening. Before the testing standardized questions were asked about the medical history, a clinical examination of the skin of the hands, arms, face and neck was performed in all players independent of the history as well as an examination of those areas indicated by the individual player’s history. Patch testing was performed with our baseline series supplemented with a work series representing the environment of the ice hockey players in the 26 teams including substances and products such as tapes, protective equipment, balms and remedies used by the physiotherapist [1]. The 72 patch test preparations were applied onto IQ Chambers (Chemotechnique Diagnostics, Vellinge, Sweden), which were attached to the back and reinforcement was made with Scanpor tape (Norgesplaster A/S, Vennesla, Norway). The test strips were removed after occlusion for 48h and the tests were read by a dermatologist on day 3 (D3) according to the International Contact Dermatitis Research Group classification [2].
Our case, a 35-year-old man, had a history of allergic rhinitis in the summer time. He had not suffered from any skin disease until the previous summer, when he got an itching rash on his dorsal feet. He suspected a new pair of rubber slippers as the cause of his skin problems. When he ceased using them, the skin problems went away. At examination immediately prior to the patch testing, no skin lesions were detected.
Discussion
At the patch test reading on D3 in the sports center 6 contact allergies were registered in our player (Table 1).
| Test substance | Test concentration % w/w | Reading day 3 |
| Diethyl thiourea | 1 | +++ |
| Methyldibromoglutaronitrile | 0.5 | +++ |
| Aluminum chloride hexahydrate | 10 | +++ |
| Thiuram mix | 1 | ++ |
| Fragrance mix I | 8 | + |
| Fragrance mix II | 14 | + |
| Oxidized linalool | 6 | (+) |
| Oxidized limonene | 3 | (+) |
Table 1: Positive patch test results on the day 3 reading and simultaneous reactions to 2 oxidized fragrance materials. All substances were tested in petrolatum.
The positive reaction to Diethyl Thiourea (DET) was impressive. The reaction was vesiculo-bullous, oedematous and significantly elevated and a spreading several centimetres outside the test area was noted (Figure 1).
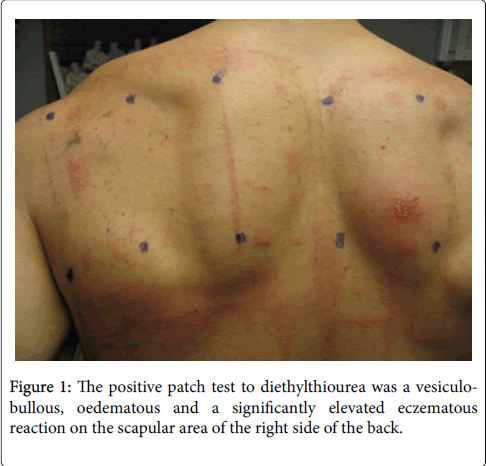
Figure 1: The positive patch test to diethylthiourea was a vesiculobullous, oedematous and a significantly elevated eczematous reaction on the scapular area of the right side of the back.
Furthermore, starting less than 24 h after the patch test application, itching erythematous, multiforme-like lesions appeared on the extremities. On D3, several erythematous-oedematous areas varying in size from a few centimeters to 10 cm2 were noted (Figure 2).

Figure 2: Erythematous, multiforme-like, itching lesions appeared on the extremities less than 24 hrs after the patch test application.
These erythematous multiforme-like lesions were interpreted as a manifestation of a systemic allergic contact dermatitis secondary to the patch tested DET. In these rare situations we usually give systemic corticosteroids to prevent further spreading, alleviate the symptoms, and to heal the dermatitis. As systemic corticosteroids are considered as doping, we treated him with topical clobetasol propionate for several days. In this way the lesions slowly disappeared and the symptoms faded, so he could play in the next game 2 days after the patch test reading.
Systemic allergic contact dermatitis seems to be an extremely rare complication after patch testing. It has been reported after testing with some textile disperse dyes [3] but not after testing with DET and is not noted as a complication in the chapter on Patch Testing in the latest edition of contact Dermatitis [4].
Contact allergy can manifest as erythema multiforme in a hypersensitive person exposed to the sensitizer at a sufficient dose. However, what is a sufficient dose? The decisive factors for a systemic allergic contact dermatitis to appear are the dose on the one hand and the individual degree of reactivity on the other [5]. The higher degree of reactivity, the lower dose is needed. Unfortunately a subsequent patch testing with serial dilutions of the suspected sensitizer, i.e. DET, down to a negative test reaction could not be performed due to the busy playing schedule with practices and games and that the player after the season moved to another country to continue his career there. Anyway, based on our experience with scientifically conducted systemic provocations with nickel and gold [6,7] and with frequent and regular patch testing of clinical cases with serial dilutions since decades, we think that the dose was sufficient to elicit a systemic contact dermatitis, manifesting as an erythema multiforme-like dermatitis. We assume it would have been possible to get a positive patch test reaction to concentrations below 1 ppm. The dose applied on the patch unit was 0.3 mg (0.37 mg/cm2 skin). If it is assumed that 1% of this dose (0.003 mg) has penetrated the skin and been absorbed into the systemic circulation, this dose is 100 times higher than the dose corresponding to 1 ppm (0.00003 mg). From scientific studies we know that with nickel, an oral dose 100 times higher than what is required to elicit a positive patch test is sufficient to induce systemic contact dermatitis [8].
DET is a well-known contact allergen widely used in the rubber industry, particularly in neoprene rubber. Sources most often implicated in allergic contact dermatitis are wet suits, athletic shoes and insoles, and orthopaedic braces. As it is not present in most baseline series targeted testing must be done, and tests often reveal clinically relevant contact allergies caused by neoprene rubber [9]. We believe our ice-hockey player had become sensitized by wearing neoprene slippers which also gave him a dermatitis that ceased when he stopped using the slippers.
When there were 6 contact allergies in one player false positive reactions due to an “angry back” have to be excluded. Many facts tell against such an interpretation in this case; (i) There was normal skin between the positive patch test reactions; (ii) There was a pattern with contact allergy to groups of sensitizers, i.e. to rubber with contact allergy to DET and thiuram mix, to fragrances with contact allergy to fragrance mix I and II and reactions to 2 oxidized fragrances, linalool and limonene, even if they did not totally fulfill the requirements for a clear allergic reaction; (iii) There were no positive reactions to sensitizers such as Amerchol L-101 and Caine mix II which are considered to be marginal irritants at patch testing.
Conflict of Interest
All authors declare no conflicts of interest and no sources of funding.
References
- Eriksson T, Bruze M, Engfeldt M,Tegner Y, Runeson R, et al. Contact allergies in 103 professional ice hockey players working in Sweden.
- Fregert S (1981) Manual of Contact Dermatitis, 2nd. edn. Munksgaard: Copenhagen 71-81.
- Malinauskiene L, Zimerson E, Bruze M, Ryberg M, Isaksson M (2011) The commercial textile dyes Disperse Orange 1 and Disperse Yellow 3 contain more than one allergen as shown by patch testing with thin layer chromatograms. Dermatitis22: 335-343.
- Lindberg M, Matura M (2011) Patch testing in Contact Dermatitis, 439-464, 5th edition, Duus Johansen J, Frosch PJ, Lepoittevin J-P, eds. Springer Verlag, Berlin.
- Bruze M (1994) Systemically induced contact dermatitis from dental rosin. Scand J Dent Res102: 376-378.
- Hindsén M, Spirén A, Bruze M (2005) Cross-reactivity between nickel and palladium demonstrated by systemic administration of nickel. Contact Dermatitis53: 2-8.
- Möller H, Ohlsson K, Linder C, Björkner B, Bruze M (1999) The flare-up reactions after systemic provocation in contact allergy to nickel and gold. Contact Dermatitis40: 200-204.
- Veien NK, Menné T, Maibach HI (1991) Systemically induced allergic contact dermatitis. In: Menné T, Maibach HI, eds. Exogenous dermatoses: environmental dermatitis. Boca Raton, Fl: CRC Press, 267-282.
- Dall AB, Andersen KE, Mortz CG (2012) Targeted testing with diethylthiourea often reveals clinically relevant allergic contact dermatitis caused by neoprene rubber. Contact Dermatitis67: 89-93.
Relevant Topics
- Child Health Education
- Construction Safety
- Dental Health Education
- Holistic Health Education
- Industrial Hygiene
- Nursing Health Education
- Occupational and Environmental Medicine
- Occupational Dermatitis
- Occupational Disorders
- Occupational Exposures
- Occupational Medicine
- Occupational Physical Therapy
- Occupational Rehabilitation
- Occupational Standards
- Occupational Therapist Practice
- Occupational Therapy
- Occupational Therapy Devices & Market Analysis
- Occupational Toxicology
- Oral Health Education
- Paediatric Occupational Therapy
- Perinatal Mental Health
- Pleural Mesothelioma
- Recreation Therapy
- Sensory Integration Therapy
- Workplace Safety & Stress
- Workplace Safety Culture
Recommended Journals
Article Tools
Article Usage
- Total views: 11539
- [From(publication date):
February-2016 - Dec 12, 2024] - Breakdown by view type
- HTML page views : 10853
- PDF downloads : 686