Trends in Road Traffic Accident Related Deaths in Transkei Sub-Region of South Africa (1993-2015)
Received: 20-Mar-2018 / Accepted Date: 08-May-2018 / Published Date: 16-May-2018 DOI: 10.4172/2161-1165.1000342
Abstract
Background: Deaths caused by road traffic accidents (RTA) are a serious public health problem all over the world. The South African government has been trying hard to bring its incidence down, but still it remains a major health problem. The Transkei region is a rural part of South Africa where the RTA death toll has consistently been higher than in the urban areas of South Africa.
Objective: To study the trend in deaths related to Road Traffic Accidents in the Transkei sub-region of South Africa (1993-2015).
Method: An autopsy record review study at the Forensic Pathology Laboratory at Mthatha over a period of 23 years (1993-2015).
Results: Over a period of 23 years (1993-2015), 26 855 autopsies were conducted at the Forensic Pathology Laboratory in Mthatha; 6 620 (24.65%) of these deaths were related to RTA. The average number of RTA deaths was 45.9 per 100,000 of the population per year, of which the majority (72.12%) were males. The rate of MVA-related death has decreased from 62 per 100,000 of the population in 1993 to 41.6 per 100,000 in 2015. The male-to-female ratio was 3:1. The highest number of MVA deaths, 1 215 (20.75%), occurred among males between 21 and 30 years, while among females the number in this age group was 298 (5.08%) between 1996 and 2015.
Conclusion: There is a decreasing trend of road traffic fatalities, but it is still at a very high level in the Transkei sub-region of South Africa. Every fourth (25%) victim of non-natural death is related with RTA. This situation needs to be addressed urgently.
Keywords: Road traffic accidents; Motor vehicle accidents; Collision
Introduction
About 1.2 million people die each year as a result of road traffic crashes in the world and an additional 20-50 million are injured [1]. WHO reported (2009) that road traffic injuries were the 11th cause of death worldwide and accounted for 2.1% of all deaths globally, and 23% of all deaths from injury worldwide. Road traffic accident (RTA) deaths comprised 9.3% of non-natural deaths. Between 20 and 50 million more people suffer non-fatal injuries, with many incurring a disability as a result of their injury [1]. In total, 3 280 931 deaths were recorded in South Africa between 2001 and 2006. RTA contributed 9.5% of non-natural causes of death. Deaths due to RTA increased from 2001 to 2006 in South Africa [2].
In South Africa, road traffic injuries are a leading cause of death, accounting for 27 deaths per 100,000 people compared to the global average of 10 deaths per 100,000 [3]. Road traffic injuries are the leading cause of death among young people, aged 15-29 years [1]. People aged between 15 and 44 years account for 48% of global road traffic deaths. In WHO report (2009), South Africa road traffic accident mortality in 2008 peaked in the age group 35-49 and was lowest among children aged 0-14 and youths aged 15-24 years [2]. Males are more likely to be involved in road traffic crashes than females and among young drivers, young males under the age of 25 years are almost three times as likely to be killed in car crashes as young females [1]. About three-quarters (73%) of all road traffic deaths occur among men [1]. In 2008, male mortality as a result of RTA in South Africa was more than double the female rate in all age groups, except in the age group 0-14 years [2]. Three provinces, Limpopo, Eastern Cape and Northern Cape, had the highest road traffic accident death rate [2]. Ninety percent (90%) of the world’s fatalities on the roads occur in low-and middle-income countries, even though these countries only have approximately half of the world’s vehicles [1]. The overall global increase in road traffic accident mortality is predicted to be 67% by 2020 if appropriate action is not taken [1].
There are multiple risk factors, such as fatigue, excessive speed, use of alcohol, and cell phones. Drinking and driving increases both the risk of a crash and the likelihood that death or serious injury will result [1]. Road traffic injuries in South Africa accounted for USD 10.5 billion of health service expenditure, or 3% of gross domestic product [4]. Road traffic injuries can be prevented. Government needs to take action to address road safety in a holistic manner; this requires involvement from multiple sectors [1]. The arrest of drivers under the influence of alcohol or drugs increased significantly from 56 165 in 2009-10 to 66 697 in 2010-11 [5]. A marginal decrease in traffic mortality was reported by the Department of Transport, from 28.1 per 100,000 in 2009 to 27.5 per 100,000 in 2010 [6]. A mortuary-based study by the National Injury Mortality Surveillance System in Gauteng and Durban showed that MVA reduced from 46.3 per 100,000 in 2008 to 39.7 per 100,000 in 2010 [7]. Similar trends have been reported in predominantly rural Mpumalanga province, with road traffic mortality reducing from 68.4 per 100,000 to 57.2 per 100,000 (a greater rate of decrease than nationally) [8].
South Africa’s road traffic injury risk factors are lack of pedestrian safety, alcohol misuse, aggressive driving and limited seatbelt use [9]. Sixty percent of fatal RTAs are due to the influence of alcohol [9]. Speeding is a factor in 30-50% of road traffic crashes [10]. The purpose of this study is to highlight the problem of deaths as a result of RTA in the sub-region of Transkei, South Africa, to explore some factors that are causing accidents in this region and suggest some preventive measures.
Methods
This is a retrospective descriptive study from the post-mortem registers from 1993 to 2015. It is preliminary study which raised more questions than answers. The data were collected by 4th year’s medical students as a part of their project. They were briefed thoroughly before they started collection of data. Therefore, the chances of biasness were minimized. This retrospective study on road traffic deaths were identified the problems, which could be further help in carrying out a prospective study. Mthatha Forensic pathology laboratory is the only laboratory in this region catering for more than half a million of the population in the Transkei sub-region of South Africa (Figure 1). It is attached to the Nelson Mandela academic hospital, which is the only a teaching hospital in this province. It is also attached to the Walter Sisulu University Medical School and conducts all medico-legal cases in this region of South Africa. In total 26 855 autopsies were conducted between 1993 and 2015. Of this, 6620 autopsies were related with road traffic accidents. All the data on deaths related with road traffic accidents were recorded of a period of 23 years (1993-2015). The details of names, addresses, age, gender, date of autopsy and cause of death were recorded in the post-mortem register. Fourteen forensic officers are engaged in collecting corpses round the clock from 17 police stations in four municipalities.

Figure 1: Map of Transkei sub-region of South Africa - population catered for by Forensic Pathology Laboratory indicated by a square.
These are the OR Tambo, Mhlontlo, Chris Hani and Mbashe municipal area of about 200 square kilometres (Photograph 1). The OR Tambo municipality is the largest, and covered fully by 10 police stations. Mhlontlo municipality has four police stations, there are two in Chris Hani and one belongs to Mbashe municipality. The combined population was 400,000 in 1993, which has been increasing by an average of 3% annually. The author excluded conceptus material and foetuses, as they were not indicated by age and gender in the postmortem registers. There is difficulty in determining the nature of death among collapse cases. These people are generally found dead, and forensic officers label the cause as collapse. Data were collected on a paper sheet designed with post-mortem number, year, gender, and cause of death. These data were analysed with help of computer.
Results
Over a period of 23 years (1993-2015) 26,855 autopsies were conducted at the Forensic Pathology Laboratory in Mthatha (Table 1). In 6 620 (24.65%) of these cases, the cause of death was RTA (Table 1), with males (4,775, 17.78%) outnumbering females (1,631, 30.45%) at a ratio of 2.92:1 (Table 1).
| Rank | Males (n=21 027) | Females (n=5 828) | Total (n=26 855) | |||
|---|---|---|---|---|---|---|
| Cause of death | n (%) | Cause of death | n (%) | Cause of death | n (%) | |
| 1 | Stabbing | 4 695 (17.48) | MVA | (1 631) 30.45 | MVA | 6 620 (24.65) |
| 2 | MVA | 4 775 (17.78) | Gunshot | (650) 12.13 | Stabbing | 5 205 (19.38) |
| 3 | Gunshot | 3 246 (12.09) | Poisoning | (530) 9.89 | Gunshot | 3 947 (14.70) |
| 4 | Assault | 2 477 (9.22) | Stabbing | (454) 8.47 | Assault | 2 960 (11.02) |
| 5 | Hanging | 1 443 (5.37) | Assault | (412) 7.69 | Hanging | 1 630 (6.07) |
| 6 | Drowning | 980 (3.65) | Drowning | (325) 6.07 | Drowning | 1 321 (4.92) |
| 7 | Collapse | 1 605 (5.98) | Collapse | (529) 9.87 | Collapse | 2 164 (8.06) |
| 8 | Poisoning | 621 (2.31) | Burns | (266) 4.97 | Poisoning | 1 152 (4.29) |
| 9 | Burns | 468 (1.74) | Lightning | (192) 3.58 | Burns | 762 (2.84) |
| 10 | Fall from height | 357 (1.33) | Hanging | (187) 3.34 | Fall from height | 492 (1.83) |
| 11 | Lightning | 288 (1.07) | Fall from height | (135) 2.52 | Lightning | 491 (1.83) |
| 12 | Gas suffocation | 72 (0.27) | Gas suffocation | (29) 0.54 | Gas suffocation | 111 (0.41) |
| All causes of deaths | 100 | All causes of death | 100 | All causes of death | 100 | |
Table 1: Ranks of percentage of cause of death by gender in Umtata area, South Africa 1993-2015.
There was a downward trend in deaths as a result of RTA in the Transkei sub-region of South Africa from 1993 (62/100,000) to 2015 (41.6/100,000) (Table 2 and Figure 2). The average number of RTA deaths was 45.9 per 100,000 of the population per year. It was highest (64.6/100,000) in 1994, and lowest (32.2/100,000) in 2001 (Table 2 and Figure 2). The RTA death rate decreased sharply after 1998 (59/100,000) and again in 2001 (322/100,000) (Table 2 and Figure 2). It jumped from 32.6/100,000 of the population in 2002 to 46.2/100,000 of the population in 2005 (Table 2 and Figure 2).
| Year | Estimated population | Female | Females/ 100,000 | Male |
Males/ 100,000 | Total | Total (per 10 0,000) |
|---|---|---|---|---|---|---|---|
| 1993 | 4 00,000 | 66 | 16.5 | 182 | 45.5 | 248 | 62 |
| 1994 | 412 000 | 50 | 12.1 | 216 | 52.4 | 266 | 64.6 |
| 1995 | 424 360 | 98 | 23.1 | 126 | 29.7 | 224 | 52.8 |
| 1996 | 439 091 | 85 | 19.4 | 183 | 41.9 | 268 | 61.3 |
| 1997 | 452 264 | 80 | 17.7 | 196 | 43.3 | 276 | 61 |
| 1998 | 465 832 | 67 | 14.4 | 212 | 45.5 | 279 | 59.9 |
| 1999 | 479 807 | 52 | 10.8 | 138 | 29 | 190 | 39.8 |
| 2000 | 494 201 | 61 | 12.3 | 144 | 29.1 | 205 | 41.5 |
| 2001 | 509 027 | 47 | 9.2 | 116 | 23 | 163 | 32.2 |
| 2002 | 524 298 | 40 | 7.6 | 130 | 25 | 170 | 32.6 |
| 2003 | 54 0,027 | 56 | 10.4 | 178 | 33.1 | 234 | 43.5 |
| 2004 | 556 227 | 62 | 11.1 | 166 | 30 | 228 | 41.2 |
| 2005 | 720 304 | 99 | 13.7 | 233 | 32.5 | 332 | 46.2 |
| 2006 | 741 913 | 90 | 12.1 | 194 | 26.1 | 284 | 38.3 |
| 2007 | 764 171 | 100 | 13.1 | 265 | 34.8 | 365 | 47.9 |
| 2008 | 787 096 | 79 | 10 | 245 | 31.1 | 324 | 41.2 |
| 2009 | 810 708 | 95 | 11.7 | 257 | 31.7 | 352 | 43.4 |
| 2010 | 835 030 | 106 | 12.7 | 273 | 32.8 | 379 | 45.5 |
| 2011 | 86 0,081 | 98 | 11.4 | 262 | 30.6 | 360 | 42 |
| 2012 | 885 883 | 109 | 12.3 | 282 | 31.9 | 391 | 44.2 |
| 2013 | 912 460 | 102 | 11.2 | 267 | 29.4 | 369 | 40.5 |
| 2014 | 939 833 | 100 | 10.6 | 211 | 22.6 | 311 | 33.2 |
| 2015 | 968 028 | 103 | 10.6 | 299 | 31 | 402 | 41.6 |
| Average | 648 810 | 80.2 | 12.8 | 208.2 | 33.1 | 288 | 45.9 |
Table 2: Incidence of MVA in the Mthatha area of South Africa by gender (1993 – 2015) (n=6 620).
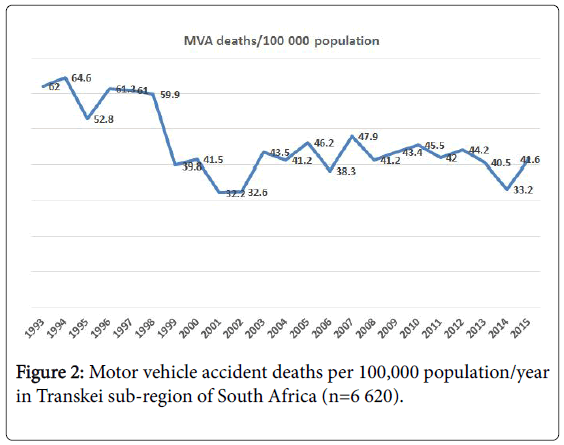
Figure 2: Motor vehicle accident deaths per 100,000 population/year in Transkei sub-region of South Africa (n=6 620).
The fall in RTA death rates has been observed among both genders (Table 2 and Figure 3). The recent average RTA death rate among males is 33.1/100,000 of the population, while among females it is 12.8/100,000 of the population in this region (Table 2). Among males it has decreased from 45.5/100,000 in 1993 to 31/100,000 of the population in 2015 (Figure 3), while among females it decreased from 16.5/100,000 in 1993 to 10.6/100,000 in 2015 (Table 2 and Figure 3).
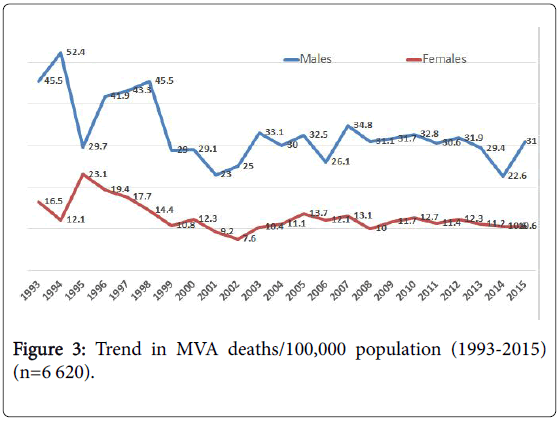
Figure 3: Trend in MVA deaths/100,000 population (1993-2015) (n=6 620).
In the young age group between 21 and 30 years, the RTA death rate is 25.84/100,000 (Table 3 and Figure 4). The highest number of deaths (43.6/100,000) is recorded in the young age group between 21 and 40 years of age (Table 3 and Figure 4). The lowest number of deaths (8.96/100,000) has been observed in the age group 61 years and above (Table 3 and Figure 4). There is a sharp decline in RTA deaths among males with advancing age, from 20.75/100,000 (21-30 years) to 0.01/100,000 (above 90 years) (Table 3 and Figure 5). Among females, the RTA death rate declined slowly with advancing age from 10.12/100,000 (21-30 years) to 0.03/100,000 (above 90 years) (Table 3 and Figure 5).
| Age group | No. of Male | % males | No. of females | % females | Total | % |
|---|---|---|---|---|---|---|
| 01-Oct | 411 | 7.01 | 263 | 4.49 | 674 | 11.51 |
| Nov-20 | 593 | 10.12 | 282 | 4.81 | 875 | 14.94 |
| 21-30 | 1215 | 20.75 | 298 | 5.08 | 1 513 | 25.84 |
| 31-40 | 817 | 13.95 | 223 | 3.8 | 1 040 | 17.76 |
| 41-50 | 552 | 9.42 | 183 | 3.12 | 735 | 12.55 |
| 51-60 | 341 | 5.82 | 151 | 2.57 | 492 | 8.4 |
| 61-70 | 188 | 3.21 | 104 | 1.77 | 292 | 4.98 |
| 71-80 | 90 | 1.53 | 85 | 1.45 | 175 | 2.98 |
| 81-90 | 35 | 0.59 | 21 | 0.35 | 56 | 0.95 |
| >90 years | 1 | 0.01 | 2 | 0.03 | 3 | 0.05 |
| Total | 4 243 | 72.5 | 1 612 | 27.5 | 5 855 | 100 |
Table 3: Age group distribution in MVA (1996-2015).
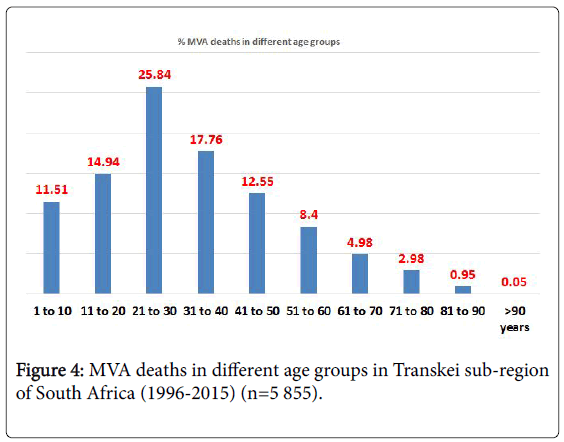
Figure 4: MVA deaths in different age groups in Transkei sub-region of South Africa (1996-2015) (n=5 855).
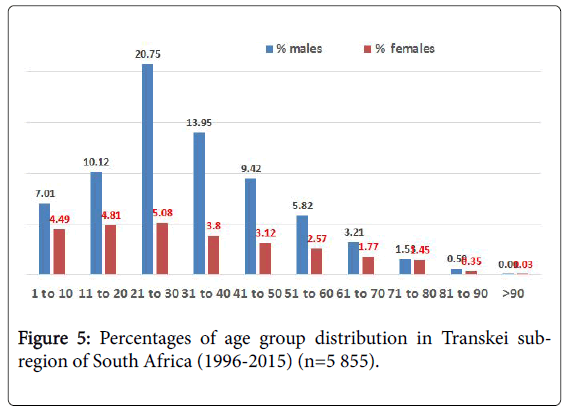
Figure 5: Percentages of age group distribution in Transkei subregion of South Africa (1996-2015) (n=5 855).
Discussion
This is the first study in rural part of South Africa that covers a study period of 23 years, using a large sample size. It justified the further research studies to be care out, and with expanded variables, so that the usefulness of this information, could be utilise for the prevention of these unnecessary deaths in this region. All unnatural deaths in the area are reported at one facility from a designated catchment area. Therefore the margin of error is minimal in this study, and this is the strength of this report. Poverty is an underlying invisible cause of death. Poverty in South Africa in general has not declined since 1994, and it is particularly severe in the former Bantustans. Rural poverty today cannot be explained as something left behind after the end of apartheid, because its causes and drivers are the same now in 2012 as they were in 1970 [11]. Transkei was a former black homeland, which was merged into South Africa when the apartheid era ended in 1994. Seventy-three percent of the rural people in the Eastern Cape were living on less than R300 per month in 2005/2006, and more than half of them on less than R220 per month [11]. The population of this region is facing a hazardous situation almost every day because of poor infrastructure in this region, among others roads, the health care system and inadequate public transport.
RTA proved to be the number one cause of non-natural deaths over the 23 years of this study in this region (Table 1). A quarter of nonnatural deaths (24.65%) are caused by RTA (Table 1), which could be preventable. Transkei is considered a rural part of South Africa. The availability of emergency care is low, as accessibility is poor, making it difficult to reach the site of an accident in the golden hour after the event. People in need of trauma care after a road crash are more likely to survive if they receive definitive care timeously [12].
Vehicle accidents are the second most frequent cause of unnatural death among males (4695-17.78%), and the first (1631-30.45%) among females (Table 1). Stabbing tops the list among males. This high number of RTA deaths is unacceptable and constitutes a heavy burden in the country’s economy. In 1998, there were 129,672 road traffic injuries that cost South Africa more than USA 1.57 billion [13]. Seven percent of road traffic injuries were fatal and accounted for 40% of the total costs; slight injuries accounted for 65% of road traffic injuries but only 23% of the cost [14]. In the Transkei sub-region of South Africa 6,620 deaths occurred as a result of RTA over a period of 23 years (1993-2015) (Table 1), and about 100,000 non-fatal injuries were inflicted in this period, costing at least several millions of rands. This economic loss to the region could be prevented by taking appropriate measures to minimize these deaths. The ‘arrive alive’ campaign must be spread throughout the year, not just in festive seasons.
South Africa can be viewed as both a first and a third-world country. On the one hand, it has glittering cities such as Cape Town, with excellent infrastructure and health care systems; on the other hand it has cities such as Mthatha (Umtata), with mud roads with multiple potholes in darkness. The mode of public transport in this region is minibus taxis, of which many are not roadworthy. Reckless driving on roads is a well-known fact [15]. This is probably the only region where mortuary vans are moving faster than ambulances, as there are a high number of non-natural deaths, and there are limited numbers of mortuary vans, so they keep on collecting corpses round the clock from 17 different police stations in an area of about 200 square kilometres (Figure 1).
The number of RTA deaths in this region has decreased about one and half times over a study period of 23 years (1993-2015), i.e. from 62 per 100,000 per year (1993) to 41.6 per 100,000 (2015) (Figure 2). The average RTA death rate is 45.9 per 100,000 per year in this study, which is nearly double (x 1.82) South Africa’s road traffic death rate (Table 2). Use of alcohol is a contributing factor to a high number of deaths on roads, especially during festive seasons such as the Christmas and Easter holidays. In 2009, alcohol-related RTAs in South Africa resulted in USD 940.6 million in damage to motor vehicles [16]. Alcohol is available everywhere in Transkei region, even on roadside, ladies are selling liquor bottles.
RTA death rate decreased sharply after 1998 and again in 2001, and then it picked up from 32.6/100,000 of the population in 2002 to 46.2/100,000 in 2005 (Table 2 and Figure 2). It is difficult to explain this trend, as many factors play a role in causing road traffic deaths: poor infrastructure, roadworthiness of vehicle, human error, alcohol use and environmental factors [17].
South Africa has the 42nd highest road mortality rate in the world, with 25.1 RTA deaths per 100,000 of the population [18]. Over 90% of RTA deaths occur in low-middle income countries, which account for 82% of the world’s population, but only 54% of the world’s registered vehicles [19]. The highest death rate was 64.6/100,000 (1994) and the lowest was 32.2/100,000 (2001) in this study (Table 2 and Figure 1).
The average RTA death rate among males is a little more than two and a half times (x2.58) that of females, i.e. males 33.1/100,000 and females 12.8/100,000 of the population in this region (Table 2 and Figure 3). It is a known fact that males are more mobile than females and more prone to risk-taking behaviour such as aggressive driving on roads, is well known in this region. Males’ consumption of alcohol and drugs is another cause of the high number of deaths [17]. The RTA death rate has reduced by almost one and a half times among both genders, i.e. from 45.5 per 100,000 (1993) to 31 per 100,000 (2015) among males, and 16.5/100,000 (1993) to 10.6/100,000 (2015) among females over the period of 23 years of this study (Table 2 and Figure 3). This similar pattern in the accident rate indicates that there may be some common factors causing these accidents. There is always a tendency to drive fast on South African roads, and it is a generally accepted norm in among peer groups to boast about it. Sometimes, males do it to impress their female partners, as they believe that they display bravery in driving fast.
Several studies have indicated that road traffic injuries are the leading cause of death among young people. Almost 60% of road traffic deaths occur among people aged 15-44 years [18]. In the young group between 11 and 40 years of age, the RTA death rate is 58.54/100,000 i.e. about 60% of total RTA deaths (Table 3). This study found that deaths resulting from RTA decrease with advancing age, i.e. after 21-30 years of age (Table 3 and Figure 4). Children under 11 years are generally passengers in the car with their parents or guardians and thus become unnecessary victims of death. Elderly people are less likely to be killed in RTA than young ones, according to this study. Only 8.96/100,000 deaths were recorded in the age group 61 and above (Table 3 and Figure 4). This is because most of people of that age are not driving cars and stay at home.
According to a 2015 report of the World Resources Institute, Johannesburg’s roads are around five times more dangerous than those of New York [18]. If one can believe this report, then Transkei roads could very well be considered five time worse than those of Johannesburg. Transkei roads lack fencing and animals that frequently cross roads are always a hazard to road users. Law enforcement agencies are not very strong. People are driving ill-maintained cars without driving licences. Licencing authorities issue licences recklessly. Medical fitness needs to be checked thoroughly before handing over any driving licence.
The Transkei region is hilly area and roads are not straight. Some people driving a car have very poor reflexes and cannot negotiate curved roads. One can predict by examining their reflexes that there are people who are not fit to drive (not to born to drive); and if they drive, it is likely to lead to accidents and death. One can advise those people that it would be safer for them not to drive to keep alive. An additional factor emerging in recent years as a cause of RTA is the cell phone. The use of a cell phone while driving is prohibited legally, but people are still using it, and it is not easy to control drivers’ behaviour in this region. Seat belts offer some protection as well, but people do not like to wear them. They only use them for short periods just to avoid a fine when police are around.
Driving is not only need a physical fitness but also a reasonable mental state. HIV infection and psychiatric disorders have a compounded the problem in RTAs. HIV infection could lead to psychiatric disorders, and psychiatric patients are more vulnerable to HIV infection [20]. An individual who is suffering from HIV/AIDs could be willing to take greater risks. It is not known how many of those involved in RTA are suffering from HIV/AIDS. A third of South African suffer from mental health disorders. More than 17 million people in South Africa are dealing with depression, substance abuse, anxiety, bipolar disorder and schizophrenia [21]. These issues might all affect people’s driving habits and road behaviour. Public education and awareness are important issues and should be included in school curricula as part of life survival skills.
Limitations
Despite the assistance of Statistics South Africa, it is difficult to estimate the actual population in South Africa as a whole accurately, as well as the region in particular, because of the awkward geographical position of serving police stations and migration numbers. The annual growth in population is estimated at 3%, which may not be strictly accurate in view of the lack of exact death and birth rates. However, the author has tried to estimate the figures as accurately as possible. The age groups were chosen for the convenience, and it has some weakness of this study, in comparing with some other established studies especially among children. However, the children are not drivers, and therefore it could be acceptable. These are raw data rates, and therefore, it has some limitation.
Conclusion
There is a decreasing trend in RTA in the Transkei sub-region of South Africa but it is still more than four and half times (x 4.59) the international average, and more than one and a half times (x 1.7) higher than the national average. On average, for every one road traffic accident death of a female, almost three (1: 2.63) males were killed in accidents in this region over the period of 23 years (1193-2015) of the study. About one-fourth of the victims of road traffic fatalities are young adults in the 21 to 30 year age group. Curbing RTA could cut economic losses to the Transkei region and the funds saved could be used to alleviate poverty in this region. Strict law enforcement, along with public education, could prevent the unnecessary road carnage in this sub-region of Transkei, South Africa.
Ethical Consideration
The author has ethical permission for collecting data and publication (approved project No. 4114/1999) from the Ethical Committee of the University of Transkei. This is an extension of earlier studies published in the American Journal of Forensic Medicine and Pathology, as well as in some South African journals and Medicine, Science and the law Journal.
Acknowledgment
The author would like to thank to all staff of the Forensic Pathology Laboratory for helping to collect data and providing information on police stations in this region. The author would also like to thank the South African Statistics Department at Mthatha for providing a population estimate.
References
- WHO (2017) Road traffic injuries - World Health Organization. WHO fact sheet.
- WHO (2009) Global status report on road safety: time for action. Geneva, Switzerland: World Health Organization.
- Statistics South Africa (2017) Road traffic accident deaths in South Africa, 2001-2006.
- Letsoalo CP (2012) State of the road safety report. Pretoria, South Africa: Road Traffic Management Corporation.
- Safety and Peace Promotion Research unit (2012) A profile of fatal injuries in Gauteng based on the National Injury Mortality Surveillance System (NIMSS).
- Safety and Peace Promotion Research Unit (2012) A profile of fatal injuries in Mpumalanga 2010 annual report for Mpumalanga based on the NIMSS.
- Road Traffic Management Corporation (2009) Road traffic report for calendar year 2009. Johannesburg, South Africa: Road Traffic Management Corporation.
- Sukai A, Seedat M, Jordaan E, Jackson D (2005) A city level study of aggressive road behaviours: magnitude, predictors, and implications for traffic safety. S Afr J Psychol 35: 244-269.
- Westaway A (2012) Rural poverty in Eastern Cape Province: legacy of apartheid or consequence of contemporary segregationism? Development Southern Africa 29: 115-125.
- Vanderschuren M, McKune D (2015) Emergency care facility access in rural areas within the golden hour? Western Cape Study. In J Health Geogr 14: 5.
- Schutte IC (2000) An estimate of unit cost of road traffic collisions in South Africa for 1998. Report No. CR-2000/4. Pretoria, South Africa: Republic of South Africa.
- Hadley KHW, Boikhutso N, Hyder AA, Bertram M, Hofman KJ (2016) Informing road traffic intervention choices in South Africa: the role of economic evaluations. Global Health Action 9: 30728.
- Meel BL (2008) Fatal road traffic accidents in the Mthatha area of South Africa, 1993-2004. SAMJ 98: 716-719.
- Truen S, Ramkolowan Y, Corrigall J, Matzopoulos R (2011) Baseline study of the liquor industry including the impact of the National Liquor Act 59 of 2003. Pretoria, South Africa: Department of Trade and Industry.
- Meel BL (2007) Trends in fatal motor vehicle accidents in Transkei region of South Africa. Med Sci Law 47: 64-68.
- Meel BL (2006) HIV/AIDS, psychiatric disorder and sexual assault in Transkei: a case report. Med Sci Law 46: 181-183.
- Chiumia S, van Wyk A (2017) Africa check. Do a third of South Africans really suffer from mental illnesses?
Citation: Meel B (2018) Trends in Road Traffic Accident Related Deaths in Transkei Sub-Region of South Africa (1993-2015). Epidemiology (Sunnyvale) 8: 342. DOI: 10.4172/2161-1165.1000342
Copyright: © 2018 Meel B. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Share This Article
Recommended Journals
Open Access Journals
Article Tools
Article Usage
- Total views: 4958
- [From(publication date): 0-2018 - Apr 26, 2025]
- Breakdown by view type
- HTML page views: 4068
- PDF downloads: 890