Transient Osteoporosis of the Talus: A Case Report
Received: 04-Mar-2019 / Accepted Date: 26-Mar-2019 / Published Date: 02-Apr-2019
Abstract
Introduction: Transient osteoporosis of the talus is a rare condition and not frequently reported in the literature. It is characterized by the acute onset of pain gradually worsening over several months. Usually, this condition affects the hip joint more than others. Radiographic changes occur, but laboratory studies are generally unremarkable. The non-operative measures had a very good outcome in the treatment of this rare condition.
Case report: This case report describes a 54-year old gentleman who presented with a disabling ankle pain without any history of previous trauma. Detailed history, clinical examination, investigation, particularly MRI was suggestive of transient osteoporosis of the talus, or what is called bone marrow edema syndrome. The patient was treated successfully with non-operative treatment.
Conclusion: Transient osteoporosis of the talus is one of the causes of the ankle pain and always should be kept in mind in the differential diagnosis of the ankle pain especially in non-traumatic conditions.
Keywords: Transient osteoporosis; Ankle joint; AVN; Talus
Introduction
Transient osteoporosis of the talus is an uncommon condition of unknown etiology that is characterized clinically by ankle pain without a history of trauma. This entity can be difficult to distinguish from osteonecrosis, stress fracture, and reflex sympathetic dystrophy syndrome (RSDS), infection, or tumor. The MR imaging findings are those of nonspecific marrow edema with a pattern of decreased signal intensity on T1-weighted images and increased signal intensity on T2- weighted images.
Case Report
A 54-year old gentleman working as a trauma physician presented to the outpatient department of the orthopedic clinic in February 2018 complaining of his right ankle pain. The pain was deep, dull aching in his right ankle and associated with swelling. Pain score was 7 out of 10 by Numeric Rating Scale. The pain was insidious and not preceded by an injury. The pain was progressive over a period of one month prior to presentation to the outpatient clinic and exaggerated with walking for long distances and relieved by rest and elevation. He is a non-smoker or non-alcoholic with unremarkable past medical and surgical histories.
Clinically the patient has antalgic gait with generalized ankle swelling compared with the contralateral side and anterior ankle joint tenderness. Using goniometer there was a painful restriction of active and passive movement of his ankle joint.
The basic blood tests including complete blood count, erythrocyte sedimentation rate, C-reactive protein, and plain radiograph were unremarkable. MRI was ordered for diagnosis and showed a diffuse decreased signal intensity of the talus on T1-weighted images and a corresponding increased signal on T2-weighted images. Associated findings included ankle joint effusion and subcutaneous edema (Figures 1 and 2).
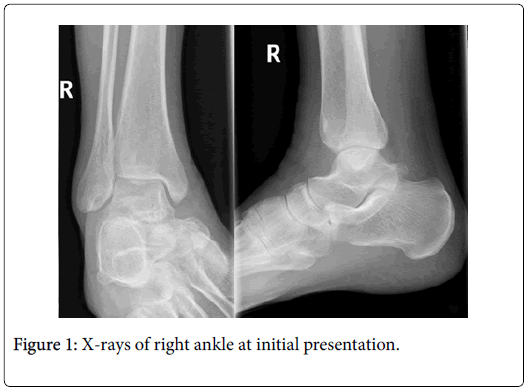
Figure 1: X-rays of right ankle at initial presentation.
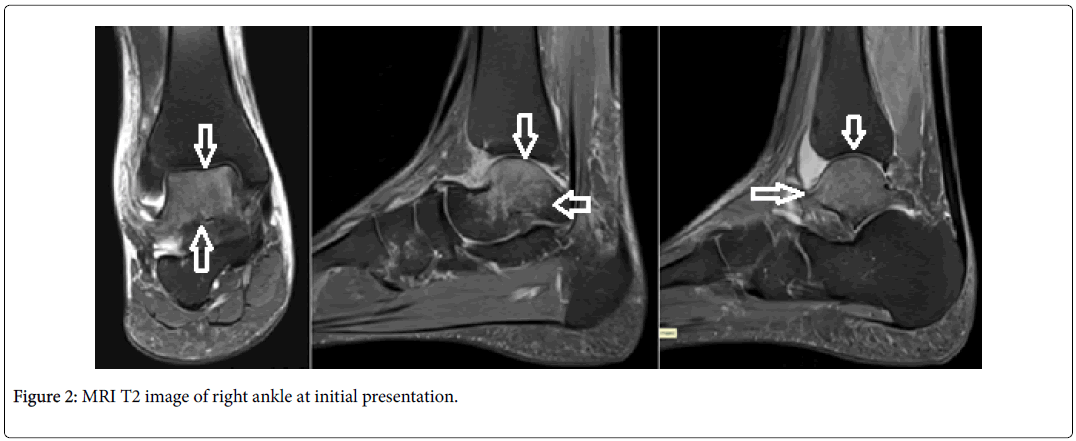
Figure 2: MRI T2 image of right ankle at initial presentation.
The patient started on non-operative treatment in the form of nonsteroidal anti-inflammatory drugs and non-weight bearing mobilization using axillary crutches for 8 weeks followed by partial weight bearing then full weight bearing after 4 months and the patient returned to full activity by 6 months. The patient showed clinical improvement regarding his pain score that improved from 7 to 4 at 2 months then 1 at 4 months and zero at 6 months follow up. Follow up MR imaging was done after 6 months which showed a complete resolution of talus marrow edema and ankle joint effusion (Figure 3).
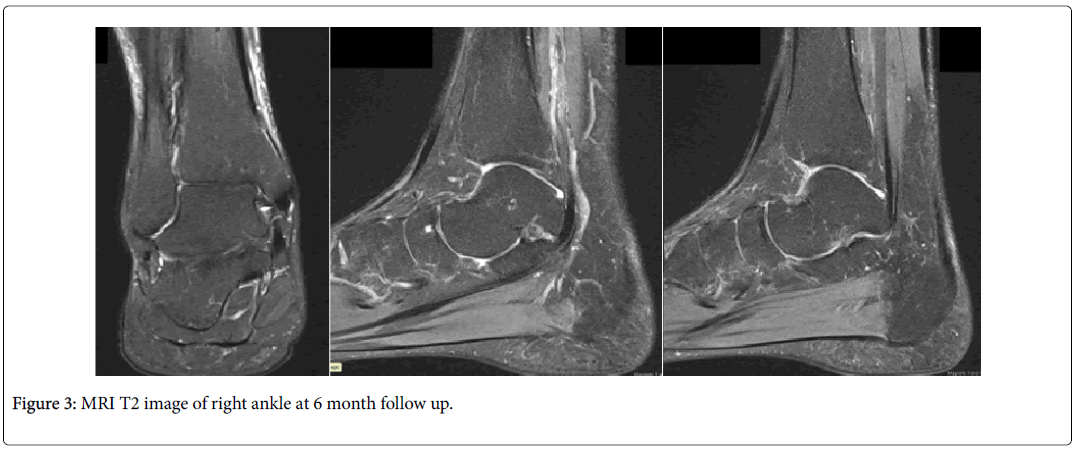
Figure 3: MRI T2 image of right ankle at 6 month follow up.
Discussion
The transient osteoporosis syndrome, alternatively transient bone marrow edema, is defined as self-limiting, of unknown etiology, painful osteopenia of the involved area [1]. It was first described in the hip during pregnancy by Curtis et al. [2]. Soon afterward, a migratory and recurrent type of transient osteoporosis was described by Duncan et al. a bone biopsy was taken in his study that showed decalcified trabecular bone [3]. The hip joint is by far the most common involved area [4]. Nevertheless, reports about the isolated involvement of talus were sparse. Calvo et al. reported 4 cases of bone marrow edema of the foot, 2 of them showed involvement of the talus [5]. Judd et al. reported a case of isolated involvement of the talus in 2000 [6]. Radke et al. studies 10 patients with foot bones edema, 8 of them involved the talus [7]. Shariff et al. studied 10 cases of transient osteoporosis of the foot, in which talus was involved in seven of them [8].
The diagnosis of transient osteoporosis of the talus is essentially by exclusion. The usual differentials are a stress fracture, spontaneous osteonecrosis, osteoarthritis, tumors and reflex sympathetic dystrophy [8]. Clinical presentation was similar in most of the cases as a sudden onset of progressive ankle pain without a history of an injury with swelling and limited range of motion [7,8].
MR Imaging is always the key for the diagnosis of transient osteoporosis especially with unremarkable ordinary radiographs. MRI finding in our case was bone marrow high signal on T2 with corresponding low signal on T1 and was consistent with the MRI findings of 5 cases of foot transient bone marrow edema reported by Calvo et al. [5].
Treatment has been discussed in the literature to a much lesser extent compared to the transient osteoporosis of the hip and knee. Non-operative treatment that includes non-weight bearing ambulation and analgesia in most of the time. Some authors suggested a protected weight bearing in a pneumatic boot for 8 weeks coupled with administration of bisphosphonates [9]. The addition of bisphosphonates reduces the average time of resolution of symptoms from 25.6 weeks down to 24 weeks for oral bisphosphonates and to 13.8 weeks for intravenous bisphosphonates [9]. Other treatments have been described include surgical core decompression [5,7] and intravenous a prostaglandin I2 analogue (Iloprost) [10,11]. Recurrence of transient osteoporosis of the foot has been reported to be as high as 44% at an average follow up of 5.75 years [9].
Conclusion
Transient osteoporosis of the talus is one of the causes of the ankle pain and always should be kept in mind in the differential diagnosis of the ankle pain especially in non-traumatic conditions. MRI imaging is a gold standard and recommended for diagnosis.
Non-operative treatment of transient osteoporosis of the talus is highly successful and should be recommended.
Conflict of Interest
No conflict of interest.
Sources of Funding
Not source of funding. No sponsors.
Ethical Approval
Institutional IRB approval was taken.
Consent
Informed consent was taken from the patient for publication of the case and related data.
Acknowledgement
I acknowledge the contribution of Dr. Moshreq Alani for his cooperation.
References
- Bramlett KW, Killian JT, Nasca RJ, Daniel WW (1987) Transient osteoporosis. Clin Orthop Relat Res 222: 197-202.
- Curtis PH, Kincaid WE (1959) Transitory demineralization of the hip in pregnancy. J Bone Joint Surg Am. 41: 1327-1333.
- Duncan H, Frame B, Frost HM, Arnstein AR (1967) Migratory osteolysis of the lower extremities. Ann Intern Med. 66: 1165-1173.
- Lakhanpal S, Ginsburg WW, Luthra HS, Hunder GG (1987) Transient regional osteoporosis: A study of 56 cases and review of the literature. Ann Intern Med 106:444-450.
- Calvo E, Alvarez L, Fernandez-Yruegas D, Vallejo C (1997) Transient osteoporosis of the foot: Bone marrow edema in 4 cases studied with MRI. Acta Orthop Scand 68: 577-580.
- Judd DB, Kim DH, Hrutkay JM (2000) Transient osteoporosis of the talus. Foot Ankle Int 21: 134-137.
- Radke S, Vispo-Seara J, Walther M, Ettl V, Eulert J (2001) Transient bone marrow oedema of the foot. Int Orthop 25: 263-267.
- Shariff SS, Baghla DP, Clark C, Dega RK (2009) Transient osteoporosis of the foot. Br J Hosp Med 70: 402-405.
- Dishan S, Ferrero A, Rose B, Goldberg A, Cullen N (2016) Bone marrow edema syndrome of the foot and ankle: mid- to long-term follow-up in 18 patients. Foot Ankle Special 9: 218-226.
- Aigner NR, Stolz MG, Petje G, Krasny C, Landsiedl F, et al. (2003) Iloprost for the treatment of bone marrow edema in the hindfoot. Foot Ankle Clinics 8: 683-693.
- Aigner N, Petje G, Steinboeck G, Schneider W, Krasny C, et al. (2001) Treatment of bone-marrow oedema of the talus with the prostacyclin analogue iloprost. An MRI-controlled investigation of a new method. J Bone and Joint Surg Br 83: 855-858.
Citation: Alburdeni S, Al-Saie J, Alhaneedi GA (2019) Transient Osteoporosis of the Talus: A Case Report. Clin Res Foot Ankle 7:287.
Copyright: © 2019 Alburdeni S, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Share This Article
Recommended Journals
Open Access Journals
Article Usage
- Total views: 4809
- [From(publication date): 0-2019 - Apr 26, 2025]
- Breakdown by view type
- HTML page views: 3997
- PDF downloads: 812