Research Article Open Access
The Effects of Homicides and Economics on Human and Social Biology: A Mental Health Challenge for a Society?
www.omicsonline.org/scholarly/mental-health-statistics-journals-articles-ppts-list.phpPaul Andrew Bourne1*, Angela Hudson-Davis2, Charlene Sharpe-Pryce3, Cynthia Francis4, Ikhalfani Solan5, Dadria Lewis3, Vivienne L. Quarrie3, Marsha Pabarue3, Shirley Nelson6, Rachael Irving7, Howard Anderson3
1Socio-Medical Research Institute, Jamaica
3Northern Caribbean University, Mandeville, Jamaica
4University of Technology, Jamaica
5South Carolina State University, USA
6Barnett’s Private Resort, Bahamas
7University of the West Indies, Mona, Jamaica
Visit for more related articles at International Journal of Emergency Mental Health and Human Resilience
Abstract
Introduction: Violence, particularly homicide, continue to plague Jamaica making it one of the countries with the highest murder rate worldwide with escalating violent espisodes which contribute to the leading cause of death among young males. Yet, homicide is not listed among the major causes of deaths in Jamaica and left out among the non-communicable diseases causing deaths. Objective: The aims of this research is to narrow the gap in the literature by evaluating from an empirical viewpoint the effects of homicides on human and social biology of theliving from a mental health perspective. Materials and Methods: The data for this study were taken from various Jamaica Government Publications including the Demographic Statistics, which provided data on mortality, population, and deaths. Jamaica Constabulary Force and Economic and Social Survey of Jamaica (ESSJ) provided the data for murders; gross domestic product per capita (i.e., GDP per capita) and suicide. Data were recorded, stored and retrieved using the Statistical Packages for the Social Sciences (SPSS) for Windows, Version 21.0. The level of significance that is used to determine statistical significance is less than 5% (0.05) at the 2-tailed level of significance. Ordinary least square (OLS) regressions were used to determine models or factors of health-care seeking behaviour. Stepwise regression was also used to the contribution of each variable leading to the final model. Results: Homicide is strongly correlated with health demands (rxy = 0.681). Of the five variables entered in the OLS regression, three emerged as factors of health-care seeking behaviour (i.e., self-reported physical illness, exchange rate and lninflation rate). This explained 83.6% of the variance in the dependent variable. Of the three factors, only one was positively correlated with dependent variable and the other two were inversely correlated with HSB. A very strong direct statistical correlation existed between the exchange rate and HSB (rxy = 0.832, P < 0.0001) with the other factors being held constant. Conclusion: Homicide must be included in human and social biology, mental health and demographic discourse as it accounts for premature deaths, psychiatric disorders and social disruptions.
Keywords
Homicide, macroeconomic variables, psychology of economics, mental health
Introduction
Violence has reached a pandemic proportion in our world. Some nations more than others are plagued by violent crimes, particularly homicide. Countries such as Jamaica, Mexico, Trinidad and Tobago, Honduras, Nicaragua, Colombia, Puerto Rico, Brazil, and El Salvador (Boxill et al., 2007; Schiller, 2011; Manwaring, 2007; Blake, 2002; Krug et al., 2002) are among those nations with the highest rates of homicide in the world. In a World Health Organization (WHO) study, it was noted by Krug et al. (2002) that youth homicide rates in Latin America and the Caribbean are the highest in the world (e.g., 84.4 per 100,000 in Colombia, 50.2 per 100,000 in El Salvador, and 41.8 in Puerto Rico compared to 11.0 per 100,000 in the United States).Furthermore, it was reported that the majority of the nations with a youth homicide rate in excess of 10 per 100,000 are in the developing world, and, that “those experiencing rapid social and economic changes” (Krug et al., 2002, p. 25). This dilemmatic situation plagues Jamaica making it one of the countries with the highest murder rate worldwide with escalating violent espisodes which contribute to the leading cause of death among young males (Smith & Green, 2007).
Jamaica is a developing country and is geographically smaller than Colombia, El Salvador and Puerto Rico yet has had youth homicides rates that are comparable and/or even greater than those nations mentioned; this violence discourse continues to be based in criminology and sociology, with little references to the epidemiology of homicide as well as the psychology of homicide on the living.Smith and Green perspective concurred when they expressed that “Youth violence has been correlated with predictors such as low self esteem, poor social problem solving skills and low empathy” (p. 419).
According to Krug et al. (2002), “The human cost in grief and pain, of course, cannot be calculated. In fact, much of it is almost invisible” (p. 3), which is possibly the justification for the empirical inquiry on the matter in the area of public health and epidemiology in the Caribbean. Despite this reality, violence is a public health phenomenon and homicide, which is a component of violence, must be studied with the same degree of intensity similar to that of noncommunicable diseases. The number of deaths caused by some noncommunicable diseases such as malignant neoplams, ischaemic heart diseases, diabetes mellitus, and hypertension are equally comparable to deaths caused by homicide in Jamaica (see Table 1). Inspite of the similarity in the number of cases of homicide and four of the major non-communicable diseases causing deaths annually in Jamaica, homicide is not listed among the 10 leading causes of deaths and is not seen as a disease. However, research provides enough evidence that homicide should be among the top causes of deaths in Jamaica as well as placed among ten non-communicable conditions causing deaths.
| Characteristics | Numbersof death by year | |||||||
|---|---|---|---|---|---|---|---|---|
| 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 | 2012 | |
| Diabetes | 1857 | 1696 | 1688 | 1709 | 1779 | 2047 | 2266 | 2177 |
| Hypertension | 888 | 907 | 1067 | 1037 | 1098 | 1079 | 1141 | 1288 |
| Ischaemic heart diseases | 849 | 1032 | 1092 | 976 | 1078 | 1044 | 1086 | 1065 |
| Malignant neoplams | 2790 | 2758 | 2883 | 2821 | 3136 | 3102 | 3270 | 3121 |
| Homicide | 1674 | 1340 | 1574 | 1601 | 1680 | 1428 | 1125 | 1095 |
| Mortality(deaths) | 15209 | 15321 | 16614 | 16445 | 15243 | 17007 | 16926 | 16999 |
Table 1: Deaths Caused by selected Non-communicable Diseases and Homicide in Jamaica, 2005-2012
The reason that many of the developing nations that are experiencing the homicide epidemic is due to the rapid socioeconomic changes, one being trust or mistrust (Krug et al., 2002). In a cross-sectional nationally representative survey of some 1,595 Jamaicans 18 years and older, Boxill et al. (2007), found that 57.1 percent of respondents reported that people are ‘somewhat trustworthy’, and only 14.1 percent indicated ‘very trustworthy’. Another cross-sectional national study of some 1,338 Jamaicans conducted at the same time as that of Boxill et al. (2007) found that interpersonal trust was 7.7 percent among Jamaicans (Powell, Bourne, & Waller, 2007). The reality is, interpersonal trust in Jamaica is relatively low and when this is added to the fact that 69.4 percent of Jamaicans indicated that the country is governed in favour of the rich; 25.1 percent said their economic situation is better off than 12 month prior and 55 percent believed that the country is ‘going in the wrong direction,’ and, 44 percent indicated that crime and violence is the leading nation problem (Powell, Bourne & Waller, 2007) with the context of the closeness between the numbers of death by homicide and certain deaths caused by non-communicable conditions, the epidemiology of homicides from a psychological perspective warrants immediate investigation.
An extensive search of the literature by the researchers did not find any study that has specifically examined the epidemiology of homicide from a pscyhological perspectives in the English-Speaking Caribbean. The aims of this research is to narrow the gap in the literature by evaluating from an empirical viewpoint the effects of homicides on human and social biology of theliving from a mental health perspective, using national data for Jamaica from 1989 to 2013.
Materials and Methods
The data for this study were taken from various Jamaica Government Publications including the Demographic Statistics, which provided data on mortality, population, and deaths. Jamaica Constabulary Force and Economic and Social Survey of Jamaica (ESSJ) provided the data for murders; gross domestic product per capita (i.e., GDP per capita) and suicide. The period for this work is from 1989 through to 2013. Data were recorded, stored and retrieved using the Statistical Packages for the Social Sciences (SPSS) for Windows, Version 21.0. The level of significance that is used to determine statistical significance is less than 5% (0.05) at the 2-tailed level of significance. Ordinary least square (OLS) regressions were used to determine models or factors of health-care seeking behaviour. Stepwise regression was also used to the contribution of each variable leading to the final model. Hence, the OLS table examine all variables at once and statistically significant variables to a final factor model of health-care seeking behaviour. As such, the contribution of each factor is a simple subtraction of the current R2 from the immediate preceding R2 value, with the first R2 representing the more or most influential factor. Prior to the use of the OLS, the researchers tested for normality of the variables (i.e., linearity and skewness including Durbin-Watson test). Those variables that skewed (negatively or positively, Sk> ± 0.8) were logged to restore normality by way of natural logarithm (loge or ln). Hence, for this, study the following variables were logged poverty, inflation, and unemployment rates, which explained the use of lnPoverty Rate; lnInflation Rate; and lnUnemployment Rate. We also tested for the likelihood of Type I and Type II Errors, by using one-tailed and twotailed test of significance. Data are compared across groups and so in cases where an analysis was made with either.
Operational Definitions
Death: The absence of life.
Study period: The studied period is 1989 to 2013, which means that there are 2.5 decades thereby. The decades are 1990-1999, and 2000-2009.
Homicide (or Murder): the unlawful killing (a crime causing death without a lawful justification) by another person(s) within a particular geopolitical zone (excluding police killings or homicides). For this work, murders represent the total number of murders for each year.
Health-Care Seeking Behaviour is the percentage of people seeking medical care.
Findings
Figure 1 depicts the annual homicides for Jamaica from 1989 to 2013. In 2013, the number of homicides stood in triple digits (1,200 or 44.2 per 100,000 population), with homicide reaching its peak in 2009 (1,680 or 62.3 per 100,000 population). Historically, the first time homicides reached triple digits in Jamaica was in 1997 (1, 034 or 40.8 per 100,000 population), and only three times since then has it fallen below 1,000 (953 or 37.2 per 100,000 population in 1998; 849 or 32.9 per 100,000 population in 1999; 887 or 34.3 per 100,000 population in 2000; 975 or 37.1 per 100,000 in 2003). In fact, since 1989 in Jamaica, homicide has been increasing at a steady rate (see Figure 1 or Annex-Table 1A).

Figure 1: Annual Homicide Rate per 100,000 population in Jamaica, 1989 to 2013
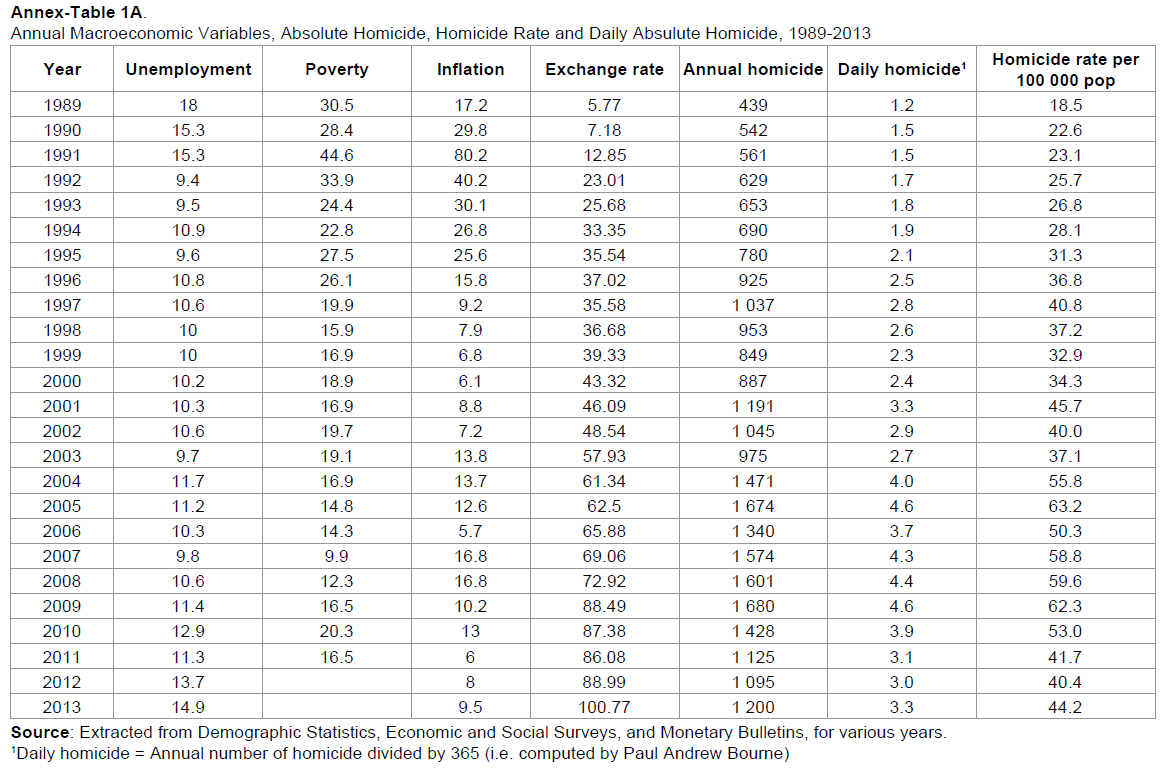
Further analysis of the homicide rate, in Jamaica, revealed that on a daily basis approximately 5 people were murderd in 2005 compared to 3 in 2013 (See Annex-Table 1A).
Table 2 presents descriptive statistics of selected macroeconomic variables, murder rate, self-reported physical illness rate (%) and HSB. Over the two and one-half decade (1989-2013), the murder rate in Jamaica stood at 18.5 per 100,000 (in 1989) to the highest of 63.2 per 100,000 (in 2009) compared to the highest inflation rate of 80.2% (in 1991) and the least of 5.7% (in 2006). Comparatively, poverty was at its highest in 1991 (44.6%) and at its lowest in 2007 (9.9%). The average murder rate for the studied period was 40.4 per 100,000 ± 13.1 per 100,000 (95% CI: 35.0–45.8 per 100,000). In 1991, poverty and inflation rates in Jamaica were at their zeniths, with poverty averaging 21.2% ± 7.9% (95% CI: 17.7–25.2) over the 25 years. Concurrently, on average, 12.2% ± 2.5% (95% CI: 11.1%– 13.4%) of Jamaicans reported a physical illness and 59.7% ± 8.98% (95% CI: 55.6–63.8) sought medical care. During the zenith of poverty and inflation in Jamaica (in 1991), 47.7% of Jamaica sought medical care, which is the second lowest in the studied period with the least being 38.6% in 1990. However, when murder was at its peak in Jamaica (in 2009), 77.1% of Jamaicans sought medical care which is unprecedent over the studied period. Simply put, when homicide rose to it zenith in 2009, 77 out of every 100 Jamaicans sought medical care compared to 54 per 100 Jamaicans in 1989 when homicide was at it lowest point (18.5 per 100,000).
| Description | Minimum | Maximum | Mean | Std. Error | Standard deviation | Skewness | 95% CI |
|---|---|---|---|---|---|---|---|
| Unemployment Rate | 9.4 | 18.0 | 11.5 | 0.45 | 2.24 | 1.53 | 10.2 – 12.2 |
| Poverty Rate | 9.9 | 44.6 | 21.2 | 1.64 | 7.87 | 1.35 | 17.7 – 25.2 |
| Inflation | 5.7 | 80.2 | 17.5 | 3.18 | 15.88 | 2.86 | 11.4 – 26.8 |
| Exchange Rate | 5.8 | 100.8 | 50.9 | 5.39 | 26.97 | 0.14 | 33.2 – 53.3 |
| Murder Rate | 18.5 | 63.2 | 40.4 | 2.72 | 13.08 | 0.28 | 35.0 – 45.8 |
| Illness Rate | 8.7 | 18.3 | 12.2 | 0.55 | 2.51 | 0.79 | 11.1 – 13.4 |
| HSB | 38.6 | 77.1 | 59.7 | 1.96 | 8.98 | -0.26 | 55.6 – 63.8 |
Table 2: Descriptive Statistics of selected Macroeconomic Variables, Murder rate, Self-reported Physical Illness Rate (%) and HSB
Table 3 presents Pearson’s Product Moment Correlation Matrix of selected macroeconomic variables (i.e., lnunemployment and lninflation), murder rate and self-reported physical illness (in %). Murder, self-reported physical illness (in %), lnunemployment rate and lninflation rate are statisticall correlated with HSB. A strong positive statistical relationship existed between HSB and murder rate (rxy = 0.763, P < 0.0001) compared to a moderate inverse relationship HSB and lninflation rate (rxy = -0.675, P < 0.0001). On the other hand, weak negative correlations emerged between HSB and illness rate (rxy = -0.494, P = 0.011) and HSB and lnunemployment rate (rxy = -0.414, P = 0.031). The direct statistical correlation between HSB and murder rate means that when the murder rate increases in Jamaica, please demand more health care service, which is indicating a rise in psychological and/or psychiatric conditions owing to murders. However, a rise in cost of living see an inverse relationship in HSB. Such a findings denotes that there is a substitution effect of food and other materials items for health care services in periods of high cost of living. However, the rise in cost of living do not influence self-reported physcial illness (P = 0.169). On the other hand, a rise in unemployment is associated with an increase in self-reported physcial illness (rxy = 0.621, P = 0.001), with the relationship being a moderately strong one.
| HSB* | murder Rate | illness | lnUnemployment rate | lnInflation rate | ||
|---|---|---|---|---|---|---|
| Pearson Correlation | HSB | 1.000 | 0.763 | -0.494 | -0.414 | -0.675 |
| Murder rate | 0.763 | 1.000 | -0.311 | -0.340 | -0.461 | |
| Self-reported Physical Illness (in %) | -0.494 | -0.311 | 1.000 | 0.621 | 0.220 | |
| lnUnemployment rate | -0.414 | -0.340 | 0.621 | 1.000 | 0.350 | |
| lnInflation rate | -0.675 | -0.461 | 0.220 | 0.350 | 1.000 | |
| Sig. (1-tailed) | HSB | . | <0.0001 | 0.011 | 0.031 | <0.0001 |
| Murder rate | <0.0001 | . | 0.085 | 0.066 | 0.018 | |
| Self-reported Illness (in %) | 0.011 | 0.085 | . | 0.001 | 0.169 | |
| lnUnemployment rate | 0.031 | 0.066 | 0.001 | . | 0.060 | |
| lnInflation rate | <0.0001 | 0.018 | 0.169 | 0.060 | . | |
| N | 24 | 24 | 24 | 24 | 24 | |
Table 3: Pearson’s Product Moment Correlations of selected Macroeconomic Variables, Self-reported Physical Illness Rate, Murder Rate per 100,000 population, Health-Care Seeking Behavior (in%)
Table 4 presents an OLS regression of selected macroeconomic variables, murder rate and physical illness rate on Health-Care Seeking Behaviour. Of the four variables entered into the model at once (i.e., two macroeconomic variables, homicide rate and selfreported physical illness rate), two variables emerged as factors of health-care seeking behaviour of Jamaicans (F [4, 20] = 13.860, P < 0.0001). The two factors (homicide rate and inflation rate) accounted for 72 percent of the variance in health-care seeking behaviour of Jamaicans (adjusted R2). Homicide is positively correlated with health-care seeking behaviour and inflation is inversely correlated with health care demands. On further examination of Table 1, homicide is strongly correlated with health demands (rxy = 0.681) with all other variables being held constant and inflation was -0.592. Simply put, homicide positively affected the health demands of Jamaica, which cannot be said for reporting a physical illness. On the other hand, when the cost of living increases, Jamaicans demand less health care services. However, the correlations between selfreported physical illness and HSB and lnunemployment rate are spurious relationships.
| Unstandardized Coefficients | Standardized Coefficients | t | P | 95% Confidence Interval | |||||
|---|---|---|---|---|---|---|---|---|---|
| B | Std. Error | Beta | Lower - Upper | Zero-order | Partial | ||||
| Constant | 63.115 | 17.685 | 3.569 | 0.003 | 25.624 - 100.606 | ||||
| Murder Rate | 0.330 | 0.089 | 0.514 | 3.723 | 0.002 | 0.142 - 0.518 | 0.763 | 0.681 | |
| lnUnemployment Rate | 4.555 | 8.206 | 0.088 | 0.555 | 0.586 | -12.841 - 21.952 | -0.414 | 0.137 | |
| lnInflation Rate | -5.267 | 1.794 | -0.403 | -2.936 | 0.010 | -9.069 - -1.464 | -0.675 | -0.592 | |
| Self-reported Illness Rate | -1.075 | 0.546 | -0.301 | -1.971 | 0.066 | -2.232 - 0.081 | -0.494 | -0.442 | |
R2 = 0.776, Adjusted R2 = 0.720
Std. Error = 4.75, Durbin-Watson = 1.8
Table 4: OLS regression of selected Macroeconomic Variables, Murder Rate and Physical Illness Rate on Health-Care Seeking Behaviour
Using Stepwise OLS, homicide accounting for 56 percent (i.e., Adjusted R2) of the variance in health demand of Jamaicans (F [1, 23] = 26.440, P < 0.0001) compared to logged inflation rate of 12.3 percent (i.e., Adjusted R2; (F [1, 23] = 22.553, P < 0.0001).
Table 5 presented an OLS regression of selected macroeconomic variables and self-reported physical illness on a dependent variable, health-care seeking behaviour (i.e., HSB). For this OLS model, we substituted murder rate with the exchange rate because there was heterodasticity with both variables. With both variables being independent variables in a single model, biased estimates would be created and therefore only one can be placed as an independent variable at a time. Therefore, of the five variables entered in the OLS regression, three emerged as factors of health-care seeking behaviour (i.e., self-reported physical illness, exchange rate and lninflation rate). This explained 83.6% of the variance in the dependent variable. Of the three factors, only one was positively correlated with dependent variable and the other two were inversely correlated with HSB. A very strong direct statistical correlation existed between the exchange rate and HSB (rxy = 0.832, P < 0.0001) with the other factors being held constant. It should be noted here that the correlation between self-reported physical illness and HSB was accommodated by the introduction of the exchange rate, making the exchange rate an intervening variable. With all other factors being held constant, the statistical association between self-reported physical illness and HSB is a moderately negative one (rxy = -0.535). This means that people tend to demand less medical care services, when self-reported physical illness are high and vice versa.
| Unstandardized Coefficients | Standardized Coefficients | 95 % Confidence Interval | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Model | B | Std. Error | Beta | P | Lower - Upper | Zero-order | Partial | |||
| Constant | 31.666 | 17.475 | 0.090 | -5.580 - 68.912 | ||||||
| Self-reported illness (in %) | -1.024 | 0.418 | -0.286 | 0.027 | -1.915 - -0.134 | -0.494 | -0.535 | |||
| Exchange Rate | 0.274 | 0.047 | 0.671 | 0.000 | 0.173 - 0.374 | 0.854 | 0.832 | |||
| Mortality Rate | 0.034 | 0.022 | 0.156 | 0.148 | -0.014 - 0.081 | 0.247 | 0.366 | |||
| lnInflation Rate | -3.552 | 1.509 | -0.272 | 0.033 | -6.769 - -0.335 | -0.675 | -0.519 | |||
| lnUnemployment Rate | 7.528 | 6.846 | 0.145 | 0.289 | -7.063 - 22.119 | -0.414 | 0.273 | |||
R2 = 0.877, Adjusted R2 = 0.836
Std. Error = 3.64, Durbin-Watson = 2.4
Table 5: OLS regression of selected Macroeconomic Variables and Self-reported Physical Illness on Health-Care Seeking Behaviour
Of the four selected macroeconomic variables entered in an OLS regression (Table 6), two emerged as factors of the murder rate (F[5, 19] = 24.3, P < 0.0001). The two factors accounted for 81.0% (i.e., adjusted R2) of the variability in the dependent variable, murder rate. A positively strong statistical correlation existed between the exchange and murder rates (rxy = 0.723, P < 0.0001) compared to the moderately inverse one between lnpoverty rate and murder rate (rxy = -0.614, P = 0.004), in each case the other independent variable being held constant. However, when Stepwise OLS was used to determine the strength of each of the two factors on the dependent variable, the exchange rate contributed 73.8% and 5.3% for lnpoverty rate.
| Model | Unstandardized Coefficients | Standardized Coefficients | P | 95.0% Confidence Interval | Zero-order | Partial | |
|---|---|---|---|---|---|---|---|
| B | Std. Error | Beta | Lower - Upper | ||||
| Constant | 58.713 | 24.183 | 0.026 | 7.908 - 109.519 | |||
| Exchange Rate | 0.342 | 0.077 | 0.613 | 0.000 | 0.180 - 0.504 | 0.866 | 0.723 |
| lnUnemployment Rate | 7.706 | 8.503 | 0.095 | 0.377 | -10.157 - 25.570 | -0.286 | 0.209 |
| lnInflation Rate | 4.485 | 2.540 | 0.224 | 0.094 | -0.851 - 9.821 | -0.448 | 0.384 |
| lnpoverty Rate | -21.710 | 6.585 | -0.548 | 0.004 | -35.544 - -7.876 | -0.805 | -0.614 |
R2 = 0.844, Adjusted R2= 0.810
Std. Error = 3.64, Durbin-Watson = 1.4
Table 6: OLS regression of selected Macroeconomic Variables on Murder Rate
Discussion
This current research examined the effects of homicides on human biology from a mental health perspective, using national data for Jamaica from 1989 to 2013. This was done in order to narrow the gap in the literature by evaluating this public health issue from an empirical viewpoint. The results from this research shows that since 1989 homicide in Jamaica has steadily increased and without appropriate interventions to reduce these rates, this issue will be irreversible. In 2013, the population of Jamaica was 2.715 million people (World Bank, 2013). However, deaths from homicide are at an alarming rate for a country the size of Jamaica. This study computed that in 1989, the homicide rate in Jamaica was 18.5 per 100,000 and this rose to 44.2 per 100,000 in 2013, with rates being 55.8 per 100,00 ≤ homicide rate ≤ 62.3 per 100,000 for the periods 2003 to 2009. In absolute number, 761 more murders were committed in 2013 compared to 1989, which represents a 138.9%. Global homicide rate in 2000 was 8.8 per 100,000 (Krug et al., 2005, p. 10) cpmared to 34.3 per 100,000 in Jamaica (current study) and 32.1 per 100,000 in low-to-middle income countries (Krug et al., 2005, p. 10). The homicide rate in the developing world including Jamaica is at least twice that in high-income nations (14.4 per 100,000, Krug et al., 2005, p. 10), offering an insight of where Jamaica’s emphasis ought to be. The writings are on the wall, Jamaica is experiencing a homicide epidemic which is worse than HIV/AIDS dilemma that is the thrust of many public health specialists and policy makers and this requires empirical investigations as well as public health interven.
Although the research provided the evidence necessary for policy makers and public health researchers to develop intervention strategies to effectively reverse this trend there is more work that is required to pinpoint the more urgent needs in addressing this issue. Smith & Green (2007), claimed in their research that crime and violence, in Jamaica, poses a significant treat to the health and well-being of the society and that these activities imposes significant costs, which includes death, injuries and mental distress, directly or indirectly on the population (Green & Smith, 2007). This study offers empirical insight to what Smith & Green (2007) forward as we found that homicide is positively influencing health demand. Homicide is health cost as when murders occur the living seeking both public and private health care, which is a public expenditure on health and increased demand on the health sector.
A 2013 report on homicide rates in the United States was 16,238 or 5.2 per 100,000 (Murphy, Xu, & Kochanek, 2013) compared to 1 200 or 44.2 per 100,000 in Jamaica. Based on the study in the US, deaths that were directly linked to firearms was 11,068 or 3.6 per 100,000 (Murphy, Xu, & Kochanek, 2013). Although these numbers are high they are significantly lower than that which was made evident through the current research. There is little attention paid to those that are left to morn the loss of loved ones (i.e., friends, family, spouse, etc). The homicide survivors are left behind to cope with various issues such as “economic stressors, stigmatization, fear of recurrence, anxiety when encountering reminders of the event, negative beliefs about themselves or feelings of guilt (Zinzow, Rheingold, Hawkins et al., 2009). This research is unearthing that homicide is not only resulting in premature death, there is a human and social biology to the homicide reality as murders are directly influence health seeking behaviour among the living. Clearly embedded in the positive correlation between homicide and health care seeking behaviour is the psychology of murders on the human biology of the living. Furthermore, the pressures could increase the risk for mental health problems such as post-traumatic stress disorder (PTSD) and other psychiatric disorders (Zinzow et al., 2009), which are parcelled in the social biology for the living.
The current study expands previous research on homicides by demonstrating the association between poverty, inflation and murder rates. During the years when inflation and poverty were at their highest so was the rates for murder. Interestingly, the was also an increase in the percentages of Jamaicans who sought medical care during the period when the murder and inflation rates were elevated. There were limitations in determining the correlation between the health-care seeking behaviors of the population under study and whether the change in behavior was due to the rise in inflation and poverty or due to address their mental health conditions resulting from homicides. In Bourne’s study, it was reported that although there is a steady increase of illness over the years, there is a significant correlation between the lack of “seeking medical care and the inflation rate” (Bourne, 2009). Bourne’s study revealed the association betweeen mortality and the pervasiveness of poverty, especially in rural communities (Bourne, 2009).
Green & Smith (2007), reported that a disproportionate amount of Jamaica’s gross domestic product (GDP) is allocated for violence related issues. It is estimated that Jamaica spends over J$ 15 billion dollars on health care cost each year, with violence related issues costing roughly 700 million Jamaican dollars (J$) (Green & Smith, 2007). This type of spending restricts the country’s abililty to compete on the global platform (Green & Smith, 2007). With the present study showing a direct correlation between homicide and health care seeking behaviour as well as the exchange rate and health care demand, murder is not only a mental health cost it is also a health care cost to the society as well as the reduced productivity from the lost humans. Homicide further limits the amount that is allocated for education, food, etc as resources but be diverted services including the need for psychiatrists, psychologists, social workers, medical practitioners, and buildings for care of the family of the deceased.
As evident from the current research, there is clearly an increase in the cost of living, however, there is increases in unemployment, which may be directly link to the rise in the number of physical illness. The surge in the number of self-reported illnesses may be a result of those unable to affort care or their illness may be related to the cost of living increases, poverty and unemployment. Undeniably, chronic poverty, unemployment and rising violence and can levy a heavy price on those that are directly impacted by these societal changes (Green & Smith, 2007). The present study revealed that self-reported illnesses increase on changes in the socio-economic status. Lower SES can significantly affect those that are more vulnerable to these changes, such as the elder, children, those who have attained lowever educational status (Rieder & Elbert, 2013). It is clear and the evidence points to the need to take action to assess the physical and mental health needs of this population under study and to assess the socio-ecological factors that could hinder intervention to address this important public health issue.
Conclusion
Published data on ten leading causes of deaths in Jamaica by the Statistical Institute of Jamaica has never included homicides among non-communicable conditions such as hypertension, diabetes mellitus, Ischaemic heart diseases and malignant neoplasm. Ironically though is the number of deaths caused by homicide in many instances are more than mortality by hypertension and Ischaemic heart diseases; yet the not ten causes of deaths include Ischaemic heart diseases, hypertension and diabetes mellitus. Clearly, homicide is a non-communicable conditions and must be included among the public health discussion on health matters. Furthermore, with current evidence that homicide is influence the human and social biology of Jamiacans, particularly mind and body of the dead as well as the living, the time has come for the inclusion of homicide into mental health, human and social biology and demography, particularly life expectancy and social biology.
The community psychiatry resulting from homicide on human and social biology has not been evaluated by Caribbean psychiatritists or public health experts, which explains why these specialists have not placed on the psychopathology to homicide. Like non-communicable diseases such as diabetes mellitus, hypertension, neoplasm and heart diseases, there are certain risk factors that people face as it relates to homicides. The reality is, in Jamaica, homicide has been constant rising and while is it not communicable it is a non-communicable condition to which emphasis must be placed by scholars as well as psychiatrists and medical practitioners.
References
- Blake, D. (2002). Shower Posse: The most notorious Jamaica criminal organization. New York: Diamond Publishing.
- Bourne, P.A. (2009). Impact of poverty, not seeking medical care, unemployment, inflation, selfreported illness, and health insurance on mortality in Jamaica. North American Journal of Medical Science, 1(3), 99-109.
- Bourne, P.A. (2012). Murder and ill-health: A health crime phenomenon. Journal of Behavioral Health,1(2), 138-146.
- Bourne, P.A. &Solan, I. (2012). Health, violent crimes, murder and inflation: public health phenomena. Journal of Behavioral Health,1(1), 59-65.
- Boxill, I., Lewis, B., Russell, R., Bailey, A., Waller, L., James, C., et al. (2007). Political culture of democracy in Jamaica: 2006Americas barometer. Kingston: The University of the West Indies.
- Harriott, A, (ed.) (2003). Understanding crime in Jamaica: New Challenges for public policy. Kingston: University of the West Indies Press.
- Harriott, A. (2004). The Jamaican crime problem: Some policy considerations. In: Harriott A, Brathwaite F, Wortley, ed. Crime and criminal justice in the Caribbean. Kingston: Arawak Publishers, pp. 265-284.
- Harriott, A. (2008). Organized crime and politics in Jamaica: Breaking the nexus. Kingston: Canoe Press.
- Harriott, A., Brathwaite, F.,& Wortley, S. (2004). Crime and criminal justice in the Caribbean. Kingston: Arawak Publishers.
- Headley, B. (1994).The Jamaican crime scene: A perspective. Mandeville: Eureka.
- Krug,E.G., Dahlberg, L.L., Mercy, J.A., Zwi, A.B., & Lozano, R. (2002). World report on violence and health. Geneva: World Health Organization.
- Levy, H. (1996). They cry ‘respect’: Urban violence and poverty in Jamaica. Kingston: Centre for Population, Community and Social Change, Department of Sociology and Social Work, the University of the West Indies, Mona.
- Manwaring, M.G. (2007). A contemporary challenge to state sovereignty: Gangs and other illicit transnational criminal organizations in Central America, El Salvador, Mexico, Jamaica and Brazil. Washington D.C: Department of the Army.
- Murphy, S.L., Xu, J.Q., & Kochanek, K.D. (2013). Deaths:Final Data for 2010. National Vital Statistics Reports. Hyattsville, MD: National Center for Health Statistics.
- Phillips, P., &Wedderburn, J.,(ed.) (1987). Crime and violence: Causes and solutions. Kingston: Department of Government, the University of the West Indies.
- Planning Institute of Jamaica (PIOJ) &Statistical Institute of Jamaica (STATIN). (1989-2010).Jamaica Survey of Living Conditions, 1989-2010. Kingston.
- Planning Institute of Jamaica (PIOJ). (1989-2010). Economic and Social Survey of Jamaica, 1988-2009. Kingston: PIOJ.
- Powell, L.A., Bourne, P.,& Waller, L. (2007). Probing Jamaica’s Political Culture, volume 1: Main trends in the July-August 2006 Leadership and governance survey. Kingston: Department of Government, the University of the West Indies, Mona.
- Rieder, H., & Elbert, T. (2013). Rwanda – lasting imprints of a genocide: trauma, mental health and psychosocial conditions in survivors, former prisoners and their children. Conflict and Health, 7(6), 1-13.
- Schiller, D. (2011). Zeta Soldiers Launched Mexico-Style Attack in Harris County. Houston Chronicle, November 23.
- Smith, D.E., & Green, K.E. (2007). Violence among youth in Jamaica: a growing public health risk and challenge. American Journal of Public Health, 22(6), 417-424.
- Zinzow, H., Rheingold, A. A., Hawkins, A., Saunders, B. E., & Kilpatrick, D. G. (2009). Losing a loved one to homicide: Prevalence and mental health correlates in a national sample of young adults. Journal of Traumatic Stress, 22(1), 20-27.
Relevant Topics
Recommended Journals
Article Tools
Article Usage
- Total views: 22149
- [From(publication date):
June-2015 - Jul 01, 2025] - Breakdown by view type
- HTML page views : 17358
- PDF downloads : 4791