Research Article Open Access
The Correlation between Neck Pain and Hand Grip Strength of Dentists
Eman Samir Fayez*Department of Physical Therapy, Faculty of Applied Medical Science, University of Dammam, Saudi Arabia
- *Corresponding Author:
- Eman Samir Fayez
Assistant professor in department of Physical Therapy
Faculty of Applied Medical Science
University of Dammam, Saudi Arabia
Tel: 009665520682167
E-mail: dremanfayez_08@yahoo.com
Received date: March 31, 2014; Accepted date: November 17, 2014; Published date: November 21, 2014
Citation: Fayez ES (2014) The Correlation between Neck Pain and Hand Grip Strength of Dentists. Occup Med Health Aff 2:185. doi: 10.4172/2329-6879.1000185
Copyright: © 2014 Fayez ES. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use,distribution, and reproduction in any medium, provided the original author and source are credited.
Visit for more related articles at Occupational Medicine & Health Affairs
Abstract
Abstract Hand grip is the functional unit of dentists used in firm holding of instruments and tools .Muscles of hand grip supplied by cervical nerves. Dentists put their neck in high physical load for prolonged time that lead to neck pain. 54.4% of dentists in K.S.A. have neck pain and 21% drop out of their job. Objective: The main objective is to find the correlation between neck pain and hand grip in dentists of Saudi Arabia. Methodology: Subjects: 25 chronic neck pain dentists (suffering from neck pain more than 3 months) in both gender, will be selected non randomly. Their ages ranged from 25 to 40 years with normal BMI (18.5-25) will be divided into subgroups according to neck position during their work. Procedures: Pain intensity will be determined by visual analog scale (VAS), hand grip strength will be measured by Jamar hand dynamometer in kilogram (Kg) unit. Result: Among 25 dentists the result showed extremely significant correlation between neck pain and hand grip strength (direct proportional). The p value (0.0001). Discussion and conclusion: the direct proportional between neck pain and hand grip strength is due to sensory motor integration deficit or due to neuro hyper excitability.
Keywords
Neck pain; Dentist; Hand grip strength; Sensory motor integration
Introduction
Neck pain is an ache or discomfort in anatomical area between occiput and 3rd thoracic vertebra and laterally between middle margin of scapula [1]. Neck pain is considered to be chronic if the patient suffered more than 3 months [2,3]. The prevalence for neck pain varies between 16.7% and 75.1% in the general population [4]. Neck pain may be caused by; spondylosis, spinal stenosis, disc herniation, stress, poor posture, prolonged posture [5,6]. Symptoms of neck pain may include; neck soreness and headache, pain around shoulder blades, arm complaints (pain, numbness or weakness).
Dental profession is one of the occupational risk factors of neck pain [1,7]. Studies showed that neck pain starts early in dental career even during educational training [8,9]. In a recent study, 54.4% of dentists in K.S.A. had neck pain, 21.69% of them drop out of job [10].
Recently, it was shown that there is a strong relation between work duration and neck pain in the staff of dental school [11,12]. Another study reported that increasing weekly work hours has little effect on neck pain [10,13]. The most common cause of neck pain in dentists is prolonged work posture which makes high load on muscles of neck and shoulder region (trapezius more than splenius) [12]. The main working posture of dentist is in sitting, with neck flexion, shoulder elevation and upper extremity abduction and his patient supine [10,11,13,14].
Hand is the functional unit of the dentist and is used in keeping firm holding of instruments and tools [15]. Hand grip is the amount of static force that the hand can squeeze around dynamometer or an index of the power which the hand can exert [16,17]. Grip strength can be affected by gender (male>female), age(peaked at 4th decade), dominant more than non-dominant hand [16-20] .Different positions may also affect hand grip strength: elbow during measurement (extension>flexion90%), supported forearm more than unsupported and standing position more than sitting [15,21] .Grip strength used to assess functional activity of hand [22] . The measurement of hand grip strength used to detect whole upper arm strength [23]. Studies show that persons with unilateral upper limb chronic pain have strength reduction of hand grip 20-30% less than non-painful side. In addition to that, unilateral musculoskeletal pain cause delay grip initiation and relaxation [24,25].
From these literature reviews we conclude that neck pain is in high prevalence in dentists and most of them take neck flexion during their work which leads to compression of nerves supply upper limb. The hand grip is a functional unit of their carrier, No previous studies show the correlation between neck pain and hand grip of dentists. So, the purpose of our study is to correlate between neck pain and hand grip strength in dentists of K.S.A.
The Purpose of the Study
The purposes of the present study were to
•Determine the relationship between neck pain intensity and hand grip strength.
•Detect which position takes high neck pain intensity.
•Detect which position takes high grip strength.
Material and Methods
Subjects selection
A cross-sectional design of 25 chronic neck pain dentists in both gender (13 male and 12 female) from dental clinic of university of Dammam and several private clinics.
Inclusion criteria
Twenty five dentists suffered from neck pain more than three months. Both genders. Their age range from 25 to 40 years with mean age 31.32 ± 4.87 years. Normal Body mass index (18.5-25 Kg/m2)
Exclusion criteria
Sixty two dentists were excluded because they had a history of either orthopedic or neurologic diseases causing functional defect of the hand strength like: fracture, surgery of upper limb or hand, carpal tunnel syndrome, De Qurvain's syndrome or diabetes mellitus.
Sampling technique and size
None randomly convenient technique to reach the volume of 25 dentists in both genders. The sample was divided into sub groups according to the neck position during working.
Instruments
Data collection sheet which include (personal data, main neck position during working). It was used for gathering data from dentists
Visual analog scale (VAS) to measure the intensity of pain [26,27] 3- Jamar hand dynamometer to measure hand grip strength [16,17,19]. (Figure 1)
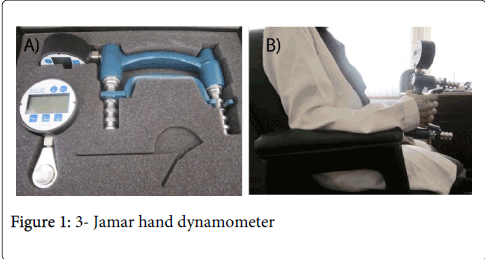
Figure 1: 3- Jamar hand dynamometer
Pre-assessment instruction
Cease taking analgesic drugs 2-3 days before examination.
Steps of assessment
1-Intensity of pain was determined by VAS rating from (0=no pain, 10=unbearable pain).
2-Grip strength was measured in the same position for all dentists : seated on chair with back support and armrest, shoulder adducted, elbow 90 degree flexed, forearm and wrist in mid position, hold the dynamometer by dominant hand (Figure 2). Therapist gave the command "squeeze around dynamometer as much as you can''. Therapist was stand in front of dentist to read the amount of force. We toke the mean of three measurements in Kg unit, with one minute rest between each squeeze to overcome fatigue [15, 16, 20].
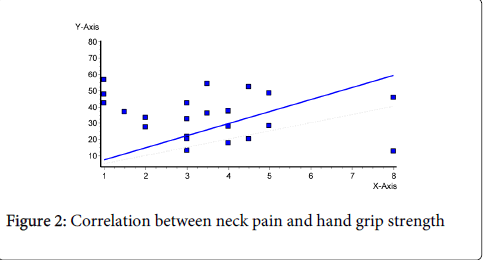
Figure 2: Correlation between neck pain and hand grip strength
Data analysis
•Data was collected from the sheet and the result of assessmentandentered to SPSS program.
•Descriptive analysis (mean, standard deviation and P value).
•Regression analysis to find the correlation between intensity of neck pain and strength of hand grip.
•One way ANOVA to compare the intensity of pain and grip strength in different neck position.
Result
Among 25 dentists, the results of this study showed extremely significant correlation between neck pain and hand grip strength (direct proportional) with p-value (0.0001) and the slope is significantly different from zero as seen in Table 1 and Figure 1. The mean of grip strength is (33.42 ± 13.05) kg .The mean of pain intensity is (3.58 ± 1.88).
| Grip strength | Neck pain | p-value |
| 33.42 ± 13.05 | 3.58±1.88 | 0.0001 |
Table 1: Correlation between neck pain and hand grip strength.
Table 2 and figure 2 showed that there was no significant difference between pain intensity in different neck positions during working of dentists by using one-way ANOVA with p-value (0.662), but neck rotation combined with flexion took the highest pain intensity (4.33 ± 3.3).
| Flexion | Side bending | Rotation with flexion | |
| Pain intensity Mean±SD |
3.55±1.7 | 3.14±1.5 | 4.33±3.3 |
| p -value | 0.662 | ||
Table 2: comparison between mean value of pain intensity in different neck position.
Table 3 and Figure 3 and 4 " showed that there was no significant difference between hand grip strength in different neck positions by using one –way ANOVA with p-value (0.196). Neck rotation also took highest hand grip strength (45.42 ± 8.67).
| Flexion | Side bending | Rotation with flexion | |
| Hand grip strength Mean±SD |
31.35±12.04 | 38.28±15.56 | 45.42±8.67 |
| p -value | 0.197 | ||
Table 3: Comparison between mean value of hand grip strength in different neck position
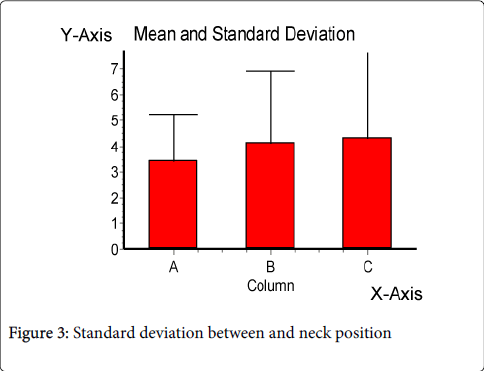
Figure 3: Standard deviation between and neck position
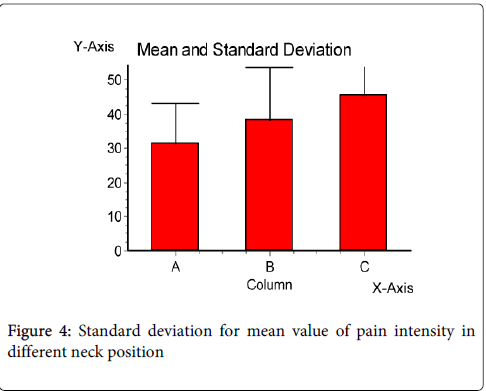
Figure 4: Standard deviation for mean value of pain intensity in different neck position
Discussion
In this study we examined the relationship between neck pain intensity and the hand grip strength in dentists. The results of the present study revealed that there was a significant positive correlation between neck pain and hand grip strength. As increase in intensity of neck pain lead to increase grip strength .This findings may be attributed to abnormality of sensory motor integration found in neck pain lead to deficit in the quality of sensory information that generate motor output. Or, may be due to sensory hyper excitability. This result agreed with Maaike et al. [28]. They measured the grip strengthin neck pain subjects and control group while carrying a 300g weight connect to (Futek, LSB200) dynamometer which measured forces applied to the object . They found that subjects with neck pain used significantly higher grip forces as compared to subjects without pain .After the initial lift object, all subject groups adapted to the lifting task by lowering their grip force level but grip force levels were still significantly higher in the subjects with pain.
Our results disagree with Michael et al. [29] who found that the grip strength decrease significantly in patients with spondylosis compared with those control group in dominant and non-dominant hand.
They clarified that increased tissue pressure arising from degenerative changes compromises myoneural conduction velocity and tissue blood flow and oxygenation .These factors interfere with the ability of the nervous system to activate hand muscles.
The results of our study showed that most pain intensity was found in rotation combined with flexion position compared with flexion and side bending positions taken by dentists. These results may be due to strain on ipsilateral facet joint which increase the risk of facet joint injury found in neck rotation [30,31]. Other study demonstrated that at 20° and 40° of rotation of the head decrease the ipsilateral neuro foraminal size up to 15% and 23%, compared with the neutral position [32] While in neck flexion they found that increase in posterior tensile force on spinal canal and soft tissue structure [33].The combination of two movements make much load on the cervical structure which cause more pain.
Conclusion
It was concluded that there was a significant direct proportional correlation between neck pain and hand grip strength in dentists.
Recommendation
It was recommended that the same study have to be conducted on larger sample size, and on different degrees of neck positions.
Acknowledgment
I would like to acknowledge Anwar Adnan M al mousa, FatimahAlwi M Al sadah, Toka Al Awazim, Noor Haddad, Noor Hassan Albrahim , Nawal Al shemary. For their great help during this research project. We also want to thank dentists how participant in our project and help us to collect data.
References
- Fejer R (2006) Neck pain (Prevalence, genetic and environmental factors). University of Southern Denmark.
- Hogg-Johnson S, van der Velde G, Carroll LJ, Holm LW, Cassidy JD, et al. (2008) The burden and determinants of neck pain in the general population: results of the Bone and Joint Decade 2000-2010 Task Force on Neck Pain and Its Associated Disorders. See comment in PubMed Commons below Spine (Phila Pa 1976) 33: S39-51.
- Jensen I, Harms-Ringdahl K (2007) Strategies for prevention and management of musculoskeletal conditions. Neck pain. See comment in PubMed Commons below Best Pract Res Clin Rheumatol 21: 93-108.
- Fejer R, Kyvik KO, Hartvigsen J (2006). The prevalence of neck pain in the world population: a systematic critical review of the literature. European spine journal: official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society. 15:834-848.
- El Keshawi A (2008) Neck pain and work-related factors among administrative and academic staff of theIslamic University of Gaza. The Islamic University-Gaza,Deanery of Higher Studies,Faculty Of Education115.
- Bernard M, Karnath M (2012) Identifying the Musculoskeletal Causes of Neck Pain. TheJournal of musculoskeletal medicine 29:82-86.
- Hush JM, Michaleff Z, Maher CG, Refshauge K (2009) Individual, physical and psychological risk factors for neck pain in Australian office workers: a 1-year longitudinal study. European spine journal : official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society. 18: 1532-1540.
- Yousef M, Al-Zain A (2009) Posture Evaluation of Dental Students 16:51-68.
- Morse T, Bruneau H, Dussetschleger J (2010) Musculoskeletal disorders of the neck and shoulder in the dental professions. See comment in PubMed Commons below Work 35: 419-429.
- Al Wazzan KA, Almas K, Al Shethri SE, Al-Qahtani MQ (2001) Back & neck problems among dentists and dental auxiliaries. See comment in PubMed Commons below J Contemp Dent Pract 2: 17-30.
- Külcü D, Güluen G, Altunok T, Küçükoulu D, Naderi S (2010) Neck and Low Back Pain Among Dentistry Staff. Turk J Rheumatol. 25:122-129.
- Finsen L, Christensen H, Bakke M (1998) Musculoskeletal disorders among dentists and variation in dental work. National Institute of Occupational Health, Department of Physiology Lerse Parkalle 105, Copenhagen DK-2100, Denmark 29:119-125.
- Harutunian K, Gargallo-Albiol J, Figueiredo R, Gay-Escoda C Ergonomics and musculoskeletal pain among postgraduate students and faculty members of the School of Dentistry of the University of Barcelona.
- Shrestha BP, Singh GK, Niraula SR (2008) Work related complaints among dentists. See comment in PubMed Commons below JNMA J Nepal Med Assoc 47: 77-81.
- Barut C, Demirel P (2012) Influense of testing posrure and elbow position on grip strength. Medical Journal of Islamic World Academy of Sciences. 20:94-97.
- Massy-Westropp NM, Gill TK, Taylor AW, Bohannon RW, Hill CL (2011) Hand Grip Strength: age and gender stratified normative data in a population-based study. See comment in PubMed Commons below BMC Res Notes 4: 127.
- Hanten WP, Chen WY, Austin AA, Brooks RE, Carter HC, et al. (1999) Maximum grip strength in normal subjects from 20 to 64 years of age. See comment in PubMed Commons below J Hand Ther 12: 193-200.
- Demura S, Aoki H, Sugiura H (2011) Gender differences in hand grip power in the elderly. Archives of Gerontology and Geriatrics 53:76-78.
- Bohannona R, Peolsson A, Westropp N, Desrosiers J, Lehmane J (2006) Reference values for adult grip strength measured with a Jamar dynamometer: a descriptive meta-analysis. Chartered Society of Physiotherapy 92: 11-15.
- Adedoyin R, Ogundapo F, Mbada C, Adekanla B, Olubusola J, et al. (2009) Refrence values for hand grip strength among healthy adults in Nigeria. Hong Kong Physiother J 27:21-29.
- Oxford KL (2000) Elbow positioning for maximum grip performance. See comment in PubMed Commons below J Hand Ther 13: 33-36.
- Langhammer B, Lindmark B, Stanghelle JK (2007) Stroke patients and long-term training: is it worthwhile? A randomized comparison of two different training strategies after rehabilitation. See comment in PubMed Commons below Clin Rehabil 21: 495-510.
- Bohannon RW (2008) Is it legitimate to characterize muscle strength using a limited number of measures? See comment in PubMed Commons below J Strength Cond Res 22: 166-173.
- van Wilgen CP, Akkerman L, Wieringa J, Dijkstra PU (2003) Muscle strength in patients with chronic pain. See comment in PubMed Commons below Clin Rehabil 17: 885-889.
- Seo NJ, Sindhu BS, Shechtman O (2011) Influence of pain associated with musculoskeletal disorders on grip force timing. See comment in PubMed Commons below J Hand Ther 24: 335-343.
- Kane RL, Bershadsky B, Rockwood T, Saleh K, Islam NC (2005) Visual Analog Scale pain reporting was standardized. See comment in PubMed Commons below J Clin Epidemiol 58: 618-623.
- Clair D, Edmondston S, Allison G (2004) Variability in pain intensity, physical and psychological function in non-acute, non-traumatic neck pain. See comment in PubMed Commons below Physiother Res Int 9: 43-54.
- Huysmans MA, Hoozemans MJ, Visser B, van Dieën JH (2008) Grip force control in patients with neck and upper extremity pain and healthy controls. See comment in PubMed Commons below Clin Neurophysiol 119: 1840-1848.
- Egwu MO, Ajao BA, Mbada CE, Adeoshun IO (2009). Isometric Grip Strength and Endurance of Patients With Cervical Spondylosis and Healthy Controls: A Comparative Study. Hong Kong Physiotherapy Journal 27:2-6.
- van Eerd M, Patijn J, Lataster A, Rosenquist RW, van Kleef M, et al. (2010) 5. Cervical facet pain. See comment in PubMed Commons below Pain Pract 10: 113-123.
- Storvik SG, Stemper BD (2011) Axial head rotation increases facet joint capsular ligament strains in automotive rear impact. See comment in PubMed Commons below Med Biol Eng Comput 49: 153-161.
- Muhle C, Resnick D, Ahn JM, Südmeyer M (2001) In Vivo Changes in the Neuroforaminal Size at Flexion-Extension and Axial Rotation Of The Cervical Spine In Healthy Persons Examined Using Kinematic Magnetic Resonance Imaging. Spine (Philadelphia, Pa 1976)26:e287-e293.
- Marshall KG (2003) THE CERVICAL SPINE. Patient Care 14:S1.
Relevant Topics
- Child Health Education
- Construction Safety
- Dental Health Education
- Holistic Health Education
- Industrial Hygiene
- Nursing Health Education
- Occupational and Environmental Medicine
- Occupational Dermatitis
- Occupational Disorders
- Occupational Exposures
- Occupational Medicine
- Occupational Physical Therapy
- Occupational Rehabilitation
- Occupational Standards
- Occupational Therapist Practice
- Occupational Therapy
- Occupational Therapy Devices & Market Analysis
- Occupational Toxicology
- Oral Health Education
- Paediatric Occupational Therapy
- Perinatal Mental Health
- Pleural Mesothelioma
- Recreation Therapy
- Sensory Integration Therapy
- Workplace Safety & Stress
- Workplace Safety Culture
Recommended Journals
Article Tools
Article Usage
- Total views: 21795
- [From(publication date):
December-2014 - Dec 04, 2024] - Breakdown by view type
- HTML page views : 17010
- PDF downloads : 4785