Research Article Open Access
Systolic Fetal Heart Murmur Detected in Fetal Phonocardiography
Kazuo Maeda1* and Hitoo Nakano21Department of Obstetrics and Gynecology, Tottori University Medical School, Yonago, Japan
2Department of Obstetrics and Gynecology, Kyushu University Faculty of Medicine, Fukuoka, Japan;
- *Corresponding Author:
- Kazuo Maeda
Department of Obstetrics and Gynecology
Tottori University Medical School
3-125, Nadamachi, Yonago
Tottoriken, 683-0835 Japan
E-mail: maedak@mocha.ocn.ne.jp
Received date: January 08, 2013; Accepted date: February 04, 2013; Published date: February 06, 2013
Citation: Maeda K, Nakano H (2013) Systolic Fetal Heart Murmur Detected in Fetal Phonocardiography. Occup Med Health Aff 1:102. doi: 10.4172/2329-6879.1000102
Copyright: © 2013 Maeda K, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Visit for more related articles at Occupational Medicine & Health Affairs
Abstract
Although clear fetal heart tones were auscultated with high-pitched tones, a sinusoidal fetal heart rate (FHR) was unable to be diagnosed, thus it was concluded that no fetal heart tone auscultation was suitable for the fetal monitoring. Fetal heart systolic period was stable and the diastolic duration varied when the FHR changed. FHR curve was traced with the triggers formed by single negative signal from the two tones of heart sound in the instantaneous FHR meter, of which microphone touching noise in FHR curve was prevented using autocorrelation heart rate meter, which made the automatic computerized FHR diagnosis successful. Fetal phonocardiography (fPCG) was studied by the tracing of fetal heart tones with the high-pass and low-cut frequency character. The oscilloscopic image recorded on a photographic film and the ink-writing record with slow-down tape technique using a data recorder achieved the recognition of high frequency component of fetal heart sound. The fetal heart tones of 105 normal pregnancies were studied and diamond shaped 100-200 Hz systolic murmur was recorded in 16.8% of the cases, which was not recorded and no cardiac abnormality was realized in the neonates after birth. Continuous wave ultrasonic record did not realize the murmur, therefore, the murmur was considered physiologically developed by the blood flow of fetal ductus arteriosus limitedly in antenatal life.
Keywords
Fetus; Heart sounds; High pitched listening; Fetal monitoring; Phonocardiography; Systolic murmur; Ductus arteriosus.
Background
The electric fetal heart activity was firstly recorded as tiny deflections on maternal limb lead electrocardifogram (ECG) by Cremer [1], direct lead fetal ECG with needle electrode by Caldeyro-Barcia et al. [2] and with scalp lead clip electrode by Hon [3]. Indirect maternal abdominal lead fetal ECG (fECG) was recorded by Maeda and Nakano [4] and others. Intrapartum fetal heart rate (FHR) was monitored by Hon [3] and Caldeyro-Barcia et al. [2] using direct lead fECG. Hammacher and Gentner [5] and Maeda [6] invented external FHR monitoring with fetal heart sound for the full fetal monitoring in 1960s. High pitched fetal heart sound listener and the fetal phonocardiography (fPCG) were studied by Maeda et al. [7] before the introduction of ultrasound diagnosis of the fetus in Japan.
Methods
Augmented fetal heart sound auscultation
A sensitive low impedance (8 ohms) dynamic microphone was connected to the step-up transformer and transistor amplifier with the peak at 60 Hz. The large corn speaker radiated low frequency fetal heart sound, of which frequency was, however, too low to listen, and disturbed by howling. Hence, the author used high pitched fetal heart sound listening device, where 1.2 kHz oscillation was modulated by low 60Hz fetal heart sound and the output was a small corn dynamic speaker (Figure 1).
Fetal phonocardiography (fPCG)
The fetal heart sound shape was studied by its records using adult standard microphone, hand-made amplifier and various recorders. The oscilloscopic image record the highest frequency range of heart sound, but needed to record with a film camera, and the record was studied after processing the film. Heat-pen or ink-writing recorder was easy to handle, but the high frequency was poorly recorded. The problem was solved by a slow-down tape technique, where the signal was recorded with TEAC R-400 data recorder (TEAC, Tokyo, Japan) with 30 in/s tape speed, and the recorded tape was reproduced with 3 in/s tape speed, where a high frequency signal was slow down to low frequency signal and recorded by the heat-pen or ink-writing recorder (Figure 2).
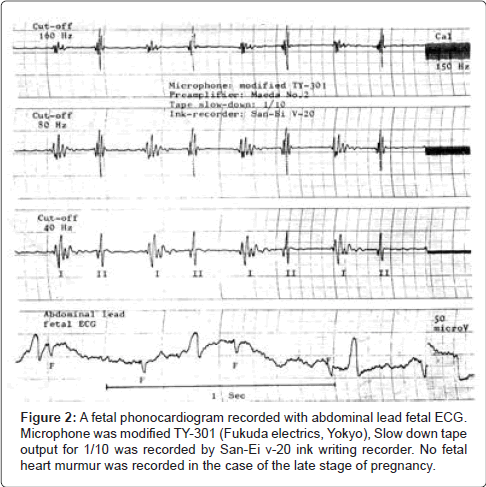
Figure 2: A fetal phonocardiogram recorded with abdominal lead fetal ECG. Microphone was modified TY-301 (Fukuda electrics, Yokyo), Slow down tape output for 1/10 was recorded by San-Ei v-20 ink writing recorder. No fetal heart murmur was recorded in the case of the late stage of pregnancy.
Fetal systolic murmur in normal fetuses
Stethoscope listening detected no fetal heart murmur. High frequency murmur was recorded with oscilloscopic fetal heart tone image with photographic film (Figure 3), or ink-writing or heat-pen recorder with the slow-down tape technique using the TEAC data (Figure 4). The fetal systolic murmur was detected in 16.8% of normal late stage pregnancy.
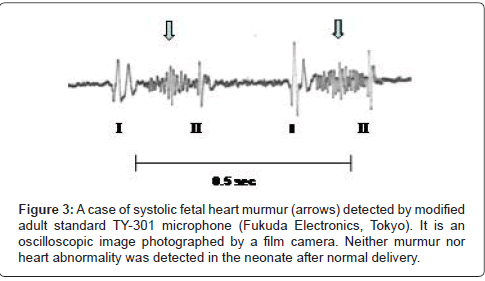
Figure 3: A case of systolic fetal heart murmur (arrows) detected by modified adult standard TY-301 microphone (Fukuda Electronics, Tokyo). It is an oscilloscopic image photographed by a film camera. Neither murmur nor heart abnormality was detected in the neonate after normal delivery.
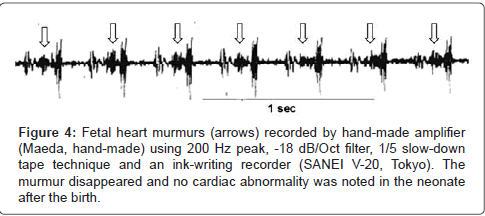
Figure 4: Fetal heart murmurs (arrows) recorded by hand-made amplifier (Maeda, hand-made) using 200 Hz peak, -18 dB/Oct filter, 1/5 slow-down tape technique and an ink-writing recorder (SANEI V-20, Tokyo). The murmur disappeared and no cardiac abnormality was noted in the neonate after the birth.
FHR monitoring with fetal heart sound
Although the FHR was initially recorded by direct lead fECG obtained by the scalp electrode was using instantaneous FHR meter, it was unable to trace the FHR during pregnancy and in early stage of labor before the rupture of membrane. Therefore, fetal heart sound on maternal abdomen was applied to trace the FHR with instantaneous FHR meter by Hammacher and Gentner [5] and Maeda [6], where single trigger was constructed from the first and second tones of fetal heart sound in a heart beat. Hammacher and Gentner [5] solved the problem by an algorithm and by flip-flop multivibrator by Maeda [6].
Since common cardiotocogram (CTG) studied by fetal heart sound accompanied the cloth touching noise of microphone, the autocorrelation FHR meter was applied to the CTG to obtain a clear noiseless tracing, and therefore it made the automated FHR diagnosis successful using fetal heart sound [7]. The beat-to-beat FHR difference was continuously recorded by fetal heart sound to study short term variability using the beat-to-beat intervals between the first vibration of the first heart tone in the instantaneous FHR meter (TOITU, Tokyo). It needed delicate manual control of the input level but it was possible to record the beat-to-beat variability [8].
Results
High pitched fetal heart sound listening device
Although the high pitched fetal heart sound of I and II tones were easily listened, recorded by common tape recorder, and transmitted by telephone line, but the listening was unable to detect sinusoidal FHR which was confirmed later by the processing of its tape recorded tone with a fetal heart rate (FHR) monitor (Toitu, Tokyo) (Figure 1), thus fetal heart auscultation did not apply to monitor the fetus to detect FHR abnormalities.
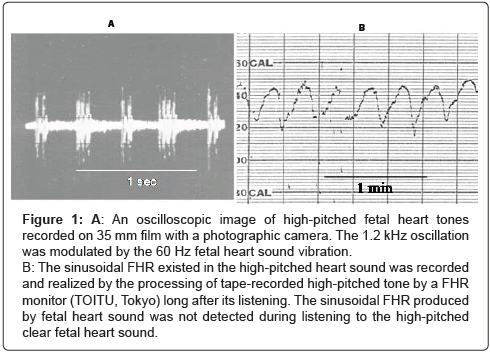
Figure 1: A: An oscilloscopic image of high-pitched fetal heart tones recorded on 35 mm film with a photographic camera. The 1.2 kHz oscillation was modulated by the 60 Hz fetal heart sound vibration. B: The sinusoidal FHR existed in the high-pitched heart sound was recorded and realized by the processing of tape-recorded high-pitched tone by a FHR monitor (TOITU, Tokyo) long after its listening. The sinusoidal FHR produced by fetal heart sound was not detected during listening to the high-pitched clear fetal heart sound.
Fetal systole and diastole
The systolic duration was almost constant, and the diastolic duration was variable in the brady- or tachycardia. (Tables 1 and 2)
| Systole (start of I tone to that of II tone) | 0.196 ± 0.020 sec (0.176 to 0.216 sec) |
| Diastole (II start to next I start) | 0.221 ± 0.028 sec ( 0.193 to 0.249 sec) |
| Beat to beat interval (I to next I) | 0.408 ± 0.038 sec (135 to 162 bpm) |
Table 1: Durations of systole, diastole, beat-to-beat changes of fetal heart sounds.
| FHR (bpm) | Systole (ms) | Diastole (ms) |
| 136 | 180 | 260 |
| 100 | 180 | 420 |
Table 2: Durations of fetal systole and diastole according to the FHR change.
Systolic fetal heart murmur
The murmur was diamond shaped and composed of 100-200 Hz vibrations during the systole between the first and second tones. The murmur was recorded in 16.8% cases of normal fetuses, and neither murmur nor heart abnormality was detected in the neonates after the delivery, whose fetuses exhibited systolic murmur (Figures 3 and 4).
Comments
Although clear fetal heart tones were listened by the high-pitched fetal heart sound listening device and its tones were easily recorded by the common tape recorder and transmitted by telephone line, the tone could detect only continuous brady- or tachycardia, but no transient FHR change, no sinusoidal FHR or no LTV change, where the FHR tracing obtained by the CTG recorded by the processing of reproduced fetal heart sound just detected valuable FHR changes. Therefore, simple auscultation of fetal heart tones should not be used in fetal monitoring even in low risk cases, where the possibility exists to produce abnormal FHR caused by sudden changes of umbilical cord, placenta or fetal environments. It was remarkable that a beat-to-beat difference was detected by fetal heart tones by the instantaneous FHR meter and the beat-to beat FHR difference recorder [8].
Fetal heart tone was composed of the first (I) and second (II) tones. Therefore, FHR counted by simple application of fetal heart sound would be twice of true FHR. The systole, however, almost stable in the fetal phonocardiogram, therefore, the FHR was recorded using single trigger signal produced by flip-flop multivibrator [8].
The cloth touching noise to microphone disappeared by the application of autocorrelation FHR meter applied to automatic diagnosis of abnormal FHR with computerized analysis [7]. Fetal systolic murmur was recorded by fPCG in many fetuses, who showed neither neonatal heart murmur nor neonatal cardiac abnormality. Since cardiac murmur is the sign of cardiac abnormality in adult patients, fetal heart murmur was also warned to be the sign of abnormal fetal cardiac function [9]. Postpartum disappearance of the systolic murmur detected during antepartum fPCG would be caused by particular fetal circulation, e.g. the blood flow in the ductus arteriosus will develop the systolic murmur, because the blood may flow ductus arteriosus in the systolic phase, the Doppler flow signal in the ductus arteriosus disappears within 48 hours after births in normal neonates [10], and neonatal persisted ductus arteriosus flow develops cardiac murmur after the birth, despite the persistent ductus arteriosus (PDA) flow maybe more complicated [11]. Although physiologic fetal systolic murmur is differentiated from pathologic cardiopathy by the disappearance of murmur after birth, cardiac murmur of the fetus may be a positive sign of a congenital heart disease in fetal heart screening. Fortunately, all of fetal systolic murmur recorded in antepartum period disappeared after birth in our studies, and therefore they were thought to be physiologic and it may be caused by fetal ductus arteriosus flow. In another view point, the murmur caused by fetal ductus arteriosus may be caused wide directivity of heart sound microphone. The record of fetal heart action with continuous wave (CW) ultrasonic Doppler fetal heart detector (Doptone, Smith-Kline, USA) recorded various fetal heart valve actions, but no blood flow through ductus arteriosus due to the narrow and unidirectional ultrasound beam in the ultrasound detector, i.e. the ultrasound beam would be radiated in the circle of 2 cm diameter covering fetal heart but not the ductus arteriosus [12], while the wide directivity of a microphone might cover the blood flow through ductus arteriosus at the same time with fetal heart valve action forming I and II heart tones. Therefore, CW ultrasonic Doppler method would be a differential diagnosis of physiological blood flow in the ductus arteriosus.
Digital technique can be used in modern fPCG, i.e. single frequency characteristics preamplifier output will be sampled with 2 ms interval and stored in computer memory. Read-out fetal heart sound is shown in computer display. Hard copy is printed out. Any analysis of the sound is performed by the computer on the read-out data. Every thing will be simplified by the computerized digital analysis.
Conclusion
Fetal heart sound auscultation should not be applied for the fetal monitoring due its poor ability to detect FHR abnormalities. FHR was recorded by instantaneous FHR meter with the single trigger formed by two tones. Beat-to-beat FHR variation was recorded with fetal heart sound too. The autocorrelation FHR meter rejected FHR tracing noises in automatic FHR diagnosis. Although fetal systolic murmur detected in the fPCG was physiologic in our cases because it disappeared after the birth and no cardiac abnormality was found in the neonate, fetal heart murmur may be a positive screening sign of congenital heart disease.
References
- Cremer M (1906) Munch Med Wschr 53: 811-813.
- Caldeyro-Barcia R, Poseiro JJ, Mendez-Bauer C, Gulin LO (1967) Effects of abnormal uterine contractions on fetal heart rate during labor. Proc V World Cong Gynecol Obstet Sydney 9-29.
- Hon EH (1968) An Atlas of Fetal Heart Rate Patterns. Harty Press, New Haven, UK.
- Maeda K, Nakano H (1969) Studies on the fetal phonocardiograpy. Proc. VIII Intern Conf Med Biol Eng, Chicago.
- Gentner O, Hammacher K (1967) An improved method for the determination of the instantaneous fetal heart frequency from the fetal phonocardiogram. Proc. VII Intern Conf Med Biol Eng.
- Maeda K (1965) Studies on the cardiotachography during labor. Proc. VI Intern Conf Med Elect Biol Eng 514-515.
- Maeda K, Arima T, Tatsumura M, Nagasawa T (1980) Computer-aided fetal heart rate analysis and automatic fetal distress diagnosis during labor and pregnancy utilizing external techniques in fetal monitoring. Medinfo 80: 1214-1219.
- Maeda K (1971) External monitoring of foetus during pregnancy and labor. Proc Workshop, IX Intern Conf Med Biol Eng Melbourne 4-9.
- Kovacs F, Kersner N, Kadar K, Hosszu G (2009) Computer method for perinatal screening of cardiac murmur using fetal phonocardiography. Comput Biol Med 39: 1130-1136.
- Drayton MR, Skidmore R (1987) Ductus arteriosus blood flow during first 48 hours of life. Arch Dis Child 62: 1030-1034.
- Bennhagen RG, Benson LN (2003) Silent and audible persistent ductus arteriosus: an angiographic study. Pediatric Cardiol 24: 27-30.
- Maeda K, Nakano H, Kimura S (1969) Pathophysiology of Fetus. Fukuoka Printing.
Relevant Topics
- Child Health Education
- Construction Safety
- Dental Health Education
- Holistic Health Education
- Industrial Hygiene
- Nursing Health Education
- Occupational and Environmental Medicine
- Occupational Dermatitis
- Occupational Disorders
- Occupational Exposures
- Occupational Medicine
- Occupational Physical Therapy
- Occupational Rehabilitation
- Occupational Standards
- Occupational Therapist Practice
- Occupational Therapy
- Occupational Therapy Devices & Market Analysis
- Occupational Toxicology
- Oral Health Education
- Paediatric Occupational Therapy
- Perinatal Mental Health
- Pleural Mesothelioma
- Recreation Therapy
- Sensory Integration Therapy
- Workplace Safety & Stress
- Workplace Safety Culture
Recommended Journals
Article Tools
Article Usage
- Total views: 18171
- [From(publication date):
February-2013 - Apr 03, 2025] - Breakdown by view type
- HTML page views : 13389
- PDF downloads : 4782