Rehabilitation of a National Taekwondo Player Following Arthroscopic Hip Surgery: Successfully Achieving a Return to Gold Medal Winning Performance Levels
Received: 20-Feb-2015 / Accepted Date: 24-Apr-2015 / Published Date: 30-Apr-2015 DOI: 10.4172/2165-7025.1000262
Abstract
This short communication outlines the successful rehabilitation of a high performance taekwondo athlete in returning to competition and becoming national champion, following right hip arthroscopy for a debilitating labral tear and impingement lesion. This case highlights a potential phased physiotherapy program that can be adapted for high level athletes in all fields, and illustrates the importance of individualized programs based on regular comprehensive assessment. The patient in question had suffered severe pain in the joint and her athletic future was in doubt; debilitating injuries of the hip can be amenable to the combination of appropriate surgical and musculoskeletal physiotherapy interventions.
Keywords: Hip arthroscopy; Rehabilitation; Sports injuries; Labral tears
Introduction
In recent years, there has been growing interest in the role of arthroscopy in the treatment of hip pathology [1]. With the evolution of minimally invasive hip surgery, labral tears have been identified as one of the main causes for pain and disability in a significant proportion of younger patients presenting with hip pain, especially athletes [2-4]. More recently there has been discussion on the overuse of arthroscopic hip surgery in treating femoral acetabular impingement [5]. Nevertheless the role of physiotherapy remains an integral part in the rehabilitation of these patients [6]. Therefore, it is vital that physiotherapists treating these patients are well informed of the important principles for recovery and return to function of these patients, thus ensuring an optimal post-operative outcome. The following account outlines a rehabilitation programme designed to successfully rehabilitate a national level taekwondo athlete with severe hip pain with resulted in the patient returning to full national competitive action.
Case Report
The patient in this case report was a 22-year-old national taekwondo athlete and was referred to our specialist clinic having experienced right hip pain for 7 years, which had significantly worsened in the last year. The patient stated the pain as 8/10 on a Numerical Rating Scale (NRS) with 10 being the worst. The main aggravating factors were weight bearing rotational movements in standing and with internal rotation (IR) and external rotation (ER) at 90 degrees hip flexion. Subjectively there was reporting of an associated clicking and locking of the hip. Magnetic Resonance Arthrography (MRA) suggested a possible labral tear; she was thus listed for arthroscopy and referred for preoperative physiotherapy assessment.
Pre-habiliation phase (pre-op)
On examination the patient displayed a pain free gait pattern with no obvious antalgic movement. Hip flexion to 130 degrees was painful at end of range movement. Extension was limited by stiffness at 20 degrees. Abduction was to 50 degrees pain free, IR in 90 degrees hip flexion was 20 degrees with some pain, ER at 90 degrees hip flexion was 30 degrees with some reproduction of groin pain. Trendelenburg sign was negative. In addition, a positive impingement test [7] and a positive FABER test [8] were elicited on the right side. Adductor squeeze test was negative for pain reproduction. The patient displayed reasonable kinetic control stability into single leg dip control with no excessive valgus collapse at the knee. Hopping on the spot was pain free on the affected side. Modified Harris hip score [9] and non-arthritic hips score [10] were 60.1 and 64.5 respectively. The patient was advised to continue with some gentle single leg proprioceptive loading via a wobble board preoperatively and to also focus on some gentle anterior hip capsule stretching via a modified Thomas Test position as pain allowed.
Operative findings
An anterior superior tear in the labrum and associated cam impingement lesion were confirmed at arthroscopy; the labrum was resected to a stable rim and the impingement lesion was excised by the Consultant Surgeon (VK).
Rehabilitation
Initial phase (0-4 weeks)
The primary focus of the initial stage of rehabilitation is to minimise pain and inflammation, to protect the repair tissue and to promote tissue healing [6]. In addition, we aim to achieve a predefined range of movement (ROM) and avoid muscle inhibition [5]. Thus, there were some important restrictions. The patient was advised to use crutches for the first 2 weeks following surgery (partial weight bearing) and then gradually progress to full weight bearing as able. In addition, hip flexion was restricted to 90 degrees and straight leg raises were avoided during this initial fortnight, to avoid irritation of the surgical area and strain on the iliopsoas. Finally, the athlete was advised to avoid internal and external rotation when in flexion for 6 weeks. This was based on consultant preference and also to minimise trauma to trimmed labrum.
A thorough musculoskeletal assessment was undertaken at the first appointment at 1 week post-op. Iliopsoas ‘snapping’ was still evident, as was adductor tenderness. Thus, static stretching of the iliopsoas (Figure 1) was initiated and an exercise regime was adopted to address the adductor discomfort, as previously described by Brukner and Khan [11]. This involved isometric loading exercises which began with squeezing a soccer ball between the ankles 30 sec (10 reps) and progressed onto squeezing the ball between the knees in crook lying (Figures 2 and 3). Furthermore Isometric strengthening exercises for the gluteus, quadriceps and hamstrings were introduced, alongside passive and active hip flexion exercise up to the 90 degree limit.
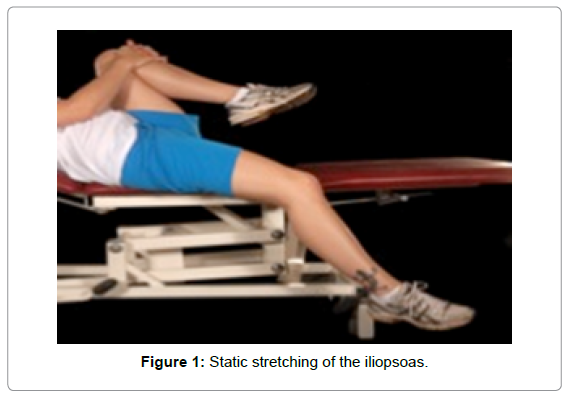
Figure 1: Static stretching of the iliopsoas.
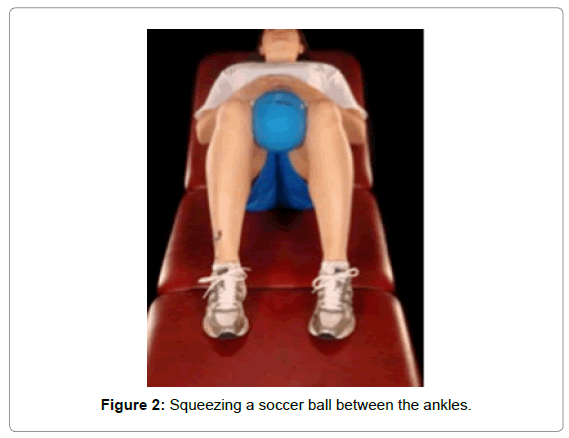
Figure 2: Squeezing a soccer ball between the ankles.
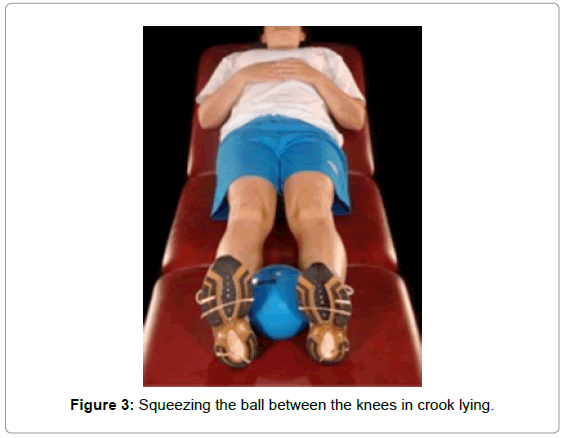
Figure 3: Squeezing the ball between the knees in crook lying.
At week 3 the patient was reassessed and was able to fully weight bear without aid. Core strength was evaluated using a single squat test, with relative weakness reflected by adduction and internal rotation of the femur [12]. Bridging exercises using both legs, abduction in side lying and straight leg raises were introduced at this stage to begin to address muscle strength. Quadruped rocking and stationary cycling without resistance were begun, with high seating to avoid excess flexion. The patient was advised to perform gentle IR and ER movements, but only with hip in neutral. As upper limb strength and conditioning is also important in taekwondo, resistance exercises using dumbbells and therabands were added to regimen. Throughout this phase the patient was instructed not to work into pain and to aim to fatigue the muscle groups.
At week 4, the above exercises were progressed as per Table 1. In addition wobble board exercises were commenced. The patient was initially instructed to single leg stand and maintain balance, progressed to single leg stand on wobble board with weights by her side to load the kinetic chain further.
| Week 0-2: | Crutches |
| Restricted hip flexion to 90 degrees | |
| Avoidance of straight leg raises | |
| Static iliopsoas stretches | |
| Static adductor exercises | |
| Isometric strengthening exercises - gluteals, quadriceps, hamstrings | |
| Week 3: | Assessment – including core strength evaluation |
| Quadruped rocking | |
| Hip rotation – in neutral | |
| Stationary cycling with no resistance and high seating | |
| Two leg bridging | |
| Upper limb – dumbells and theraband exercises | |
| Week 4: | Stationary cycling with minimal resistance for up to 20 minutes |
| Lower limb theraband exercises with light resistance | |
| Proprioceptive training with wobble board (two legs) | |
| Week 5: | Dynamic stretching of iliopsoas |
| Core strengthening exercises progressed e.g. ball exercises | |
| Single leg bridging | |
| Week 6: | Hip rotation exercises- commenced in flexion |
| Lower limb theraband exercises – resistance increased, sidestepping introduced | |
| Military press and push ups | |
| Week 7: | Assessment |
| 1/3 squats against wall with gym ball behind back | |
| Resisted external/internal rotation | |
| Bridging with gym ball | |
| Weeks 8-12: | Lunges |
| Proprioceptive training with wobble board (one leg at a time) | |
| Rowing machine | |
| Swimming | |
| Plyometrics – starting in water and gradually building intensity | |
| Week 12 +: | Sport specific training and Advanced plyometrics |
Table 1: Exercise regime from 0-12 weeks.
Intermediate phase (5-7 weeks)
The main goals in this phase are to achieve full range of motion in all planes, improve flexibility and regain strength and power progressively [5,6]. In addition the patient should achieve independence in daily activities with minimal discomfort [13]. At week 6, IR and ER of the patient was assessed in 90 degree flexion. It was found that pain (NRS =4) was a limiting factor at 45 IR and 50 ER. Dynamic stretching of the anterior hip capsule (kneeling and forward lunging) was gradually added at this stage as tolerated (Figure 4). Quadruped rocking was increased in amplitude to involve full ROM of the hip. Core strengthening exercises were increased in difficulty to include single leg bridging (Figure 5) and progressive gym ball work e.g. sitting on the ball and raising the foot off the floor or double leg squats with a ball in between the knees. Rowing exercises were introduced to maintain cardiovascular endurance. Theraband exercises were continued as in the initial phase but with increased resistance; sidestepping with therabands was encouraged to improve abductor strength [5]. To enhance upper trunk and upper limb strength, push ups and military press were started at week 5.

Figure 4: Dynamic stretching of the anterior hip capsule.
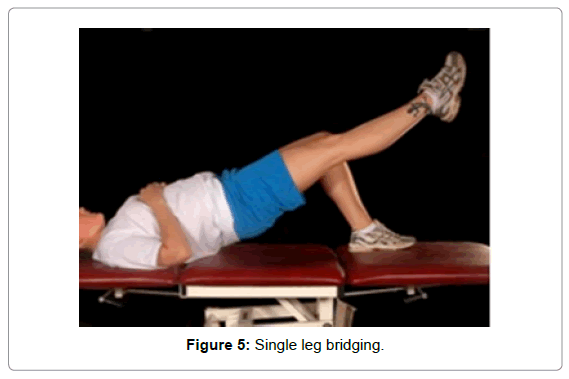
Figure 5: Single leg bridging.
At week 7, the athlete was formally reassessed. The patient demonstrated pain free flexion to 130 degrees, pain free extension to 30 degrees. Pain on NRS was scored at 2/10. Subjective reporting of ‘snapping’ in her anterior hip capsule had reduced. She scored her VAS as 1/10. Her outcome measures were MHHS-95.1 and NAHS -95 out of 100. Exercises were again progressed, as per Table 1.
Advanced Phase (8-12 weeks)
The goals of rehabilitation in this phase are to achieve a symmetrical ROM, restore muscle endurance and strength, improve cardiovascular endurance and optimise balance and proprioception [5]. The therapist should also give attention to movements of a functional nature which would involve multiple muscle groups [6]. To address these aims, resistance was enhanced for all exercises, including static biking and rowing machine. Swimming allowed significant improvement in her aerobic fitness without overloading the hip capsule. Plyometric exercises were begun at this stage, initially in water, then progressing onto skipping on dry land; plyometric exercises had a major role to play in our athlete, as many of the kicks in taekwondo require explosive power and speed. Core strengthening exercises was increased in difficulty eg: bridging with the gym ball, sit ups with the gym ball and side bridging. Proprioceptive training was advanced to single leg wobble board exercises.
Sports Specific Training 12 weeks onwards
To progress onto this particular phase the athlete needs to have achieved full ROM without pain or signs of muscle weakness. The aim is to allow a safe and effective return to premorbid levels and competition. Agility, speed and power are the core skills that a Taekwondo athlete. Thus, plyometric exercises were adapted to mimic the athlete’s kicks and jumps. These included kicking with a resistance cord or theraband around the ankle (Figure 6), forward walking and alternate leg kicks with theraband tied around the waist and pulled from behind, jumping on and off a box and single leg squats (without weights initially and then with weights). Regular discussions or even joint sessions along with the coach should be an integral part of this phase.

Figure 6: Theraband around the ankle.
Discussion
The importance of dividing rehabilitation of such patients into ‘phases’ lies in the distinct goals associated with each of them. These relate to the different healing properties of the involved tissues. ROM exercises were gradually initiated during the beginning of the rehabilitation program so as to keep the pain and inflammation of the surgical site under control. Regular reassessment and individualisation of the regimen is paramount – our patient complained about snapping and pain whilst performing straight leg raises (SLR). It is generally believed that whilst performing an SLR the forces through the hip equal 3 times the body weight and since iliopsoas is one of the primary muscles of active SLR [14] it was decided not to overload this muscle in the initial weeks. Following adequate healing, the physiotherapist can shift focus to progressively increase range of movement, strength, flexibility and improve endurance. The importance of cardiovascular fitness should be born in mind throughout the process, whilst it is imperative to add sports specific exercises which include the nonaffected limbs to achieve return to competition.
Core strength work represents a key focus in the rehabilitation regime after hip arthroscopy in the literature. Leetun et al. showed evidence that decreased core strength is one of the primary factors for lower limb injuries in athletes [15]. Along with core strength the therapist also has to focus on hip and trunk stability in this situation. In high performance athletes, a good level of core strength is assumed by all. However, unfortunately this may not be the case after periods of inactivity and cessation of training, during which core strength can dwindle significantly and rapidly. The athlete described in this case study had to withdraw from training for almost 9 months and this had severely affected her core strength. A graded program of core strengthening exercises such as that outlined above allows achievable and progressive improvement to complement hip-specific exercises.
Continuous passive movement (CPM) has been proposed as a potentially useful adjunct in such regimens. Several animal studies conducted in the past [16,17] have provided evidence that CPM leads to benefits in cartilage regeneration. Thus, applying CPM may be of benefit in patients who have had microfracture of the acetabulum. Importantly, the majority of previous studies advocating CPM in humans have focused on knees, and further studies are required to prove if CPM exerts this positive effect on the acetabular labrum. Moreover, a Cochrane review published in 2010 concluded that ‘the effects of CPM on ROM are too small to justify its use [18]. There is evidence that CPM reduces the need for subsequent manipulation under anaesthesia, however, the quality of the evidence is low and this possible benefit needs to be carefully weighed against the inconvenience and expense of CPM.’ As hip arthroscopy is generally performed as a day case in the UK, applying the CPM for 8 hours per day, over 2-4 weeks as has been advocated [13] would have been impractical. Due to these reasons we did not employ it in our regimen.
The acetabular labrum has been shown to contribute to proprioception [19].
Thus, it has been postulated that damage to the labrum can affect this function; indeed patients may exhibit sub-optimal balance when standing on one leg. For this reason, proprioceptive exercises should be given importance within any regimen following labral damage.
Plyometrics represent an important group of exercises chosen by many therapists in an athlete’s rehabilitation. The benefits of plyometrics, in conjunction with weight training, include considerable improvements in power and strength [20,21]. When considering sports specific exercises, we recognized that taekwondo involves activities like jumping and kicking which will require good flexibility, explosive power and strength; plyometrics will help achieve all this.
This patient had gained weight since stopping training, becoming 5 kg heavier than her competition weight category limit. Furthermore, high level taekwondo requires an advanced level of aerobic fitness. By individualizing her regimen to include various exercises to target cardiovascular endurance throughout her rehabilitation process, we were able to address both of these sports-specific concerns.
Outcome measures used were the Modified Harris Hip score [9] and the Non-Arthritic hip scores [10] which are both recognised outcome measures for hip arthroscopy patients. In this particular patient, both outcome measure improved by 35 points at 6 weeks, which reflects the benefit of appropriate surgical intervention and phased rehabilitation. Whilst focusing on lower limb and core strengthening, it was important not to forget that the upper limb will also need certain amount of training and conditioning. In taekwondo, upper limb strength and endurance is clearly important [22]. An athlete would need an overall body strength and conditioning program to avoid injuries and perform better. Whilst the ‘sport specific phase’ occurs about 3 months postoperatively, this refers more to the lower limb; upper limb strength can be begun as early as 2 weeks with therabands, dumbbells and progress onto push-ups and barbells in later stages. Exercises like Military press and deadlifts are useful adjuncts to progress.
Conclusion
This annotation describes an individualized, phased rehabilitation program designed for a young aspiring athlete who had ceased training due to her injury, but was able to regain national gold medal-winning performance levels. The concepts outlined here can be adapted to athletes in various fields. As hip arthroscopy continues to develop, physiotherapists need to be aware of the current evidence to inform their practice. With the appropriate surgical intervention and rehabilitation, athletes can return, and even surpass, pre-morbid performance levels.
Funding Sources
The author’s wishes to confirm that no funding was received by any means for this study.
Consent
Written consent was obtained from patient for publishing the case notes and pictures.
Acknowledgement
The author would like to thank Phillipa Adams, Physiotherapy Technical instructor for her contribution in managing this case.
References
- Khanduja V, Villar RN (2007) The arthroscopic management of femoroacetabular impingement. Knee surgery, sports traumatology, arthroscopy : official journal of the ESSKA 15:1035-1040.
- Philippon M, Schenker M, Briggs K, Kuppersmith D (2007)Femoroacetabular impingement in 45 professional athletes: associated pathologies and return to sport following arthroscopic decompression. Knee Surg Sports TraumatolArthrosc 15:908-914.
- Byrd JW, Jones KS (2004) Diagnostic accuracy of clinical assessment, magnetic resonance imaging, magnetic resonance arthrography, and intra-articular injection in hip arthroscopy patients. Am J Sports Med 32:1668-1674.
- Bedi A, Chen N, Robertson W, Kelly BT (2008) The management of labral tears and femoroacetabular impingement of the hip in the young, active patient. Arthroscopy 24:1135-1145.
- Reiman MP, Thorborg K (2015) Femoroacetabular impingement surgery: are we moving too fast and too far beyond the evidence? Br J Sports Med .
- Garrison JC, Osler MT, Singleton SB (2007) Rehabilitation after arthroscopy of an acetabularlabral tear. N Am J Sports PhysTher 2: 241-250.
- Ganz R, Parvizi J, Beck M, Leunig M, Nötzli H, et al. (2003) Femoroacetabular impingement: a cause for osteoarthritis of the hip. ClinOrthopRelatRes : 112-120.
- Margo K, Drezner J, Motzkin D (2003) Evaluation and management of hip pain: an algorithmic approach. J FamPract 52: 607-617.
- Byrd JW, Jones KS (2000) Prospective analysis of hip arthroscopy with 2-year follow-up. Arthroscopy 16:578-587.
- Christensen CP, Althausen PL, Mittleman MA, Lee JA, McCarthy JC (2003) The nonarthritic hip score: reliable and validated. ClinOrthopRelatRes : 75-83.
- Peter B, Karim K (2007) Clinical Sports Medicine. (3 edtn), McGraw-Hill Medical Publishing Division,New York.
- Willson JD, Dougherty CP, Ireland ML, Davis IM (2005) Core stability and its relationship to lower extremity function and injury. J Am AcadOrthopSurg 13: 316-325.
- Edelstein J, Ranawat A, Enseki KR, Yun RJ, Draovitch P (2012) Post-operative guidelines following hip arthroscopy. Curr Rev Musculoskelet Med 5: 15-23.
- Hu H, Meijer OG, van DieënJH, Hodges PW, Bruijn SM, et al. (2010) Muscle activity during the active straight leg raise (ASLR), and the effects of a pelvic belt on the ASLR and on treadmill walking. J Biomech 43: 532-539.
- Leetun DT, Ireland ML, Willson JD, Ballantyne BT, Davis IM (2004) Core stability measures as risk factors for lower extremity injury in athletes. Med Sci Sports Exerc 36: 926-934.
- Salter RB, Simmonds DF, Malcolm BW, Rumble EJ, MacMichael D, et al. (1980) The biological effect of continuous passive motion on the healing of full-thickness defects in articular cartilage. An experimental investigation in the rabbit. J Bone Joint SurgAm 62:1232-1251.
- Shimizu T, Videman T, Shimazaki K, Mooney V (1987) Experimental study on the repair of full thickness articular cartilage defects: effects of varying periods of continuous passive motion, cage activity, and immobilization. J Orthop Res 5:187-197.
- Harvey LA, Brosseau L, Herbert RD (2010) Continuous passive motion following total knee arthroplasty in people with arthritis. Cochrane Database Syst Rev 17: CD004260.
- Kim YT, Azuma H (1995) The nerve endings of the acetabular labrum. ClinOrthopRelatRes : 176-181.
- Arasi HA (2011) The effect of aquatic and land plyometric training on strength, sprint, and balance in young basketball players. Journal of Human Sports& Exercise6:8.
- Blakey J, BaS D (1987) The combined effect of weight training and plyometrics on dynamic leg strength and leg power. Journal of Applied Sports Science Research 1:3.
- Chiodo S, Tessitore A, Cortis C, Lupo C, Ammendolia A, et al. (2011) Effects of official Taekwondo competitions on all-out performances of elite athletes. J Strength Cond Res 25:334-339.
Citation: Punnoose A, Gallagher C, Matthews J, Khanduja V (2015) Rehabilitation of a National Taekwondo Player Following Arthroscopic Hip Surgery: Successfully Achieving a Return to Gold Medal Winning Performance Levels. J Nov Physiother 5:262. Doi: 10.4172/2165-7025.1000262
Copyright: © 2015 Punnoose A, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Share This Article
Recommended Journals
Open Access Journals
Article Tools
Article Usage
- Total views: 15757
- [From(publication date): 4-2015 - Jul 05, 2024]
- Breakdown by view type
- HTML page views: 11376
- PDF downloads: 4381