Pulmonary Adenocarcinoma, Eight Years after the Treatment of a Dedifferentiated Chondrosarcoma of the Pelvis
Received: 11-Aug-2018 / Accepted Date: 24-Aug-2018 / Published Date: 31-Aug-2018 DOI: 10.4172/2472-016X.1000126
Keywords: Chondrosarcoma; Surgery; Chemotherapy; Radiotherapy; Prognosis
Introduction
Chrondrosarcoma is the second most common primary malignant tumour of bone after osteosarcoma [1]. It most often occurs in the pelvis. Dedifferentiated chondrosarcoma is composed of two distinguishable components: low-grade chondrosarcoma components and high-grade dedifferentiated components. It represents about 10% of all chondrosarcoma. Because of the high propensity of dedifferentiated chondrosarcoma to metastasize, its treatment remains a challenge. There are very few published data on the survival of patients with dedifferentiated chondrosarcoma and more specifically, on the efficacy and role of chemotherapy, particulary in the era of modern diagnostic and treatment modalities.
Case Presentation
We report the case of a 41-year-aged man, non-smoker, with no familial history of bone tumors. On admission to our hospital, six months after he was first seen, the patient reported constant low back pain. The findings of laboratory tests were normal. Radiographs of pelvis revealed lesions with lytic characteristics on the left iliac wing. CT scan of the pelvis revealed an expansive processus of iliac wing with perforation of the cortex associated with a tissular matrix (Figure 1). A percutaneous biopsy was performed concluding to a dedifferentiated chondrosarcoma (Figures 2 and 3). Radiographs and computed tomography scans of the chest revealed no evidence of pulmonary metastases. The case was discussed in a multidisciplinary team which prescribed a preoperative chemotherapy because the tumor was jugged unresectable. The patient received two cycles of chemotherapy by PAI (Cisplatine, Adriamycine Ifosfamide) followed by a complete resection with no residual disease. An adjuvant chemotherapy was administered by three cycles of the same protocole. The patient then had a 54 Gy radiotherapy in 30 fractions of 1,8 Gy, five days per week for six weeks, confined to the tumor bed. The patient had a complete remission. He was followed-up regularly by clinical examination each three months and a semestrial body CT. A CT scan of the chest realized in January 2016 showed the presence of a pulmonary mass.
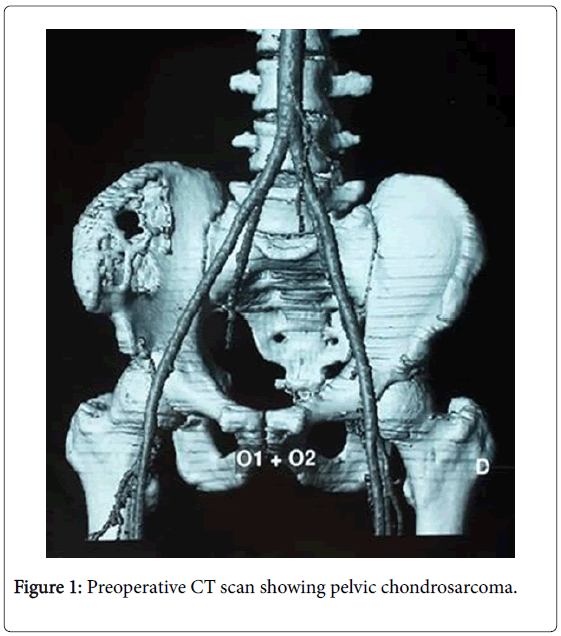
Figure 1: Preoperative CT scan showing pelvic chondrosarcoma.

Figure 2: The histological examination of the resected tumor.

Figure 3: The histological examination of the resected tumor.
A biopsy CT guided was performed. The examination of the specimen concluded to a pulmonary adenocarcinoma (CK7+, TTF1+). The tumor was judged unresectable.
Discussion
It's crucial to distinguish between conventional chondrosarcoma and dedifferentiated chondrosarcoma regarding the significant difference of prognosis.
Dedifferentiated chondrosarcoma have a poor prognosis. The overall five-year survival rate was 7.1% and the median survival time was 7.5 months [2]. Patients rarely survive for more than 2 years and died the most frequently from lung metastasis which represents the worst prognostic factor. Another important prognostic factor on local outcome is the site of the tumor. Those tumors which crossed the sacroiliac joint had a higher incidence of local recurrence compared with those at other sites. In our case, the patient is still alive after a follow-up of eight years without recurrence of his initial cancer.
Osaki et al. [3] and Kawai series [4] of pelvic chondrosarcoma showed a five-year survival rate of 65% and a ten-year survival rate of 54%. In series of Sheth et al. [5] which included sixty seven patients with pelvic chondrosarcoma reporter a ten-year survival rate of 52%. This lower survival rate may be explained by the more important number of patients with dedifferentiated chondrosarcoma in this study. The grade is an established prognostic factor in theses series which considerally enworse PFS and OS. Ten-year survival rate decrease from 97% to 14% for respectively grade-1 to grade-3 tumors.
Surgery is the corner stone of treatment especially when "carcinologic" resection with wide margins is possible. Therefore, the localization in the pelvis has a much more difficult surgical approach than the localization in the extremities due to the anatomic complexity of the pelvis and the close proximity of the tumor to surrounding neurovascular and visceral structures.
The important local recurrence rate explains the tendency to an extended surgery.
At the time of local recurrence, poor prognosis for patients with metastatic disease justifies the use of palliative treatment such as radiation therapy or other debulking procedures instead of agressive approaches to avoid long duration. For people with no metastatic disease when the local recurrence occurs, wide resection margins with extended reconstruction are justified, regarding the relatively high survival rates.
Our patient has the particularity of a much better outcome than reported in the literature. This difference can be explained by the use of perioperative chemotherapy especially when we considered the tumor as non-resectable which allowed us to perform a resection with wide margins. This attitude was sustained by a current consensus around the treatment of dedifferentiated chondrosarcoma using a multidisciplinary approach like osteosarcomas.
Although this consensus is not based on prospective studies, many retrospective ones suggests better outcomes for patients who received chemotherapy compared with those who were treated by surgery only. In 1995, Benjamin et al. presented their experience with continuous infusion with Doxorubicin and Cisplatine or ifosfamide with methotrexate in 15 patients with dedifferentiated chondrosarcoma and reported a 51% relapse-free-survival rate at 30 months of follow-up, but this study hadn’t a group control and that constrained us to compare these findings to the results of Johnson et al. [6] who proposed in 1986 surgery only for all the 17 patients with resectable dedifferentiated chondrosarcoma and who reported a median time to relapse of 5 months and median survival of 10 months. All patients died within 25 months. In 2000, Mitchell et al. [7] series of 22 patients with dedifferentiated chondrosarcoma treated in the Royal Orthopaedic Hospital in Birmingham, England, found a median survival of 9 months for patients who had only a surgical treatment versus 14 months for those who had also chemotherapy. The five-year survival was 18% for the group control and 36% for the chemotherapy group.
Otherwise, since prognosis depends essentially on lung metastasis, the control of metastasis appears to be interesting even though, there is a lack of evidence to a benefit of chemotherapy for metastatic dedifferentiated chondrosarcoma. Its use remains controversial, in particular when we consider toxicities of chemotherapy for older patients with metastatic disease and an inappropriate performance status.
A large retrospective study [8] including 337 patients whose 71 had metastasis, published in 2007 by the European Musculo-Skeletal Oncology Society (EMSOS) concluded on not statistically significant difference between best supportive care and palliative chemotherapy for the metastatic subset, which could also be attributed to the difference of performance status at diagnosis.
Radiotherapy is an alternative in the therapeutic arsenal not only on palliative purpose for local recurrence particularly with pelvic localisations or non-resectable tumors where it can help to avoid ulceration and slow down tumor progression but also as an adjuvant treatment after en bloc resection with positive margins even if these tumors are thought to be radioresistant regarding to the low mitotic index and relatively anaerobic matrix environment.
Conclusion
In spite of progress in imaging, surgical techniques and adjuvant chemotherapy, the prognosis of dedifferentiated chondrosarcoma remains poor. The 5 years overall survival is less than 10%. There is a hope to improve the outcomes with the new era of biologic therapies and advances in molecular genetics. There is no cases reported in the literature with a metachronous pulmonary cancer.
Conflicts of Interest
None.
References
- Damron TA, Ward WG, Stewart A (2007) Osteosarcoma, chondrosarcoma and Ewing's Sarcoma: National Cancer Data Base Report. Clin Orthop Relat Res 459: 40–47
- Dickey ID, Rose PS, Fuchs B, Wold LE, Okuno SH, et al. (2004) Dedifferentiated chondrosarcoma: the role of chemotherapy with updated outcomes. J Bone Joint Surg Am 86-A: 2412–2418
- Ozaki T, Hillmann A, Lindner N, Blasius S, Winkelmann W (1997) Chondrosarcoma of the pelvis. Clin Orthop Relat Res 337: 226–239
- Kawai A, Healey JH, Boland PJ, Lin PP, Huvos AG, et al. (1998) Prognostic factors for patients with sarcomas of the pelvic bones. Cancer 82: 851–859.
- Sheth DS, Yasko AW, Johnson ME, Ayala AG, Murray JA, et al. (1996) Chondrosarcoma of the pelvis. Prognostic factors for 67 patients treated with definitive surgery. Cancer 78: 745–750.
- Johnson S, Tetu B, Ayala AG, Chawla SP (1986) Chondrosarcoma with additional mesenchymal component (dedifferentiated chondrosarcoma). Cancer 58: 278–286
- Mitchell AD, Ayoub K, Mangham DC, Grimer RJ, Carter SR, et al. (2000) Experience in the treatment of dedifferentiated chondrosarcoma. J Bone Joint Surg Br 82-B: 55–61
- Grimer RJ, Gosheger G, Taminiau A, Biau D, Matejovsky Z, et al. (2007) Dedifferentiated chondrosarcoma: Prognostic factors and outcome from a European group. Eur J Cancer 43: 2060–2065.
Citation: Fahmi M, Amina M, Mouna A, Khalil EB, Khedija M, et al. (2018) Pulmonary Adenocarcinoma, Eight Years after the Treatment of a Dedifferentiated Chondrosarcoma of the Pelvis. J Orthop Oncol 4: 126. DOI: 10.4172/2472-016X.1000126
Copyright: © 2018 Fahmi M, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Share This Article
Recommended Journals
Open Access Journals
Article Tools
Article Usage
- Total views: 3622
- [From(publication date): 0-2018 - Feb 10, 2025]
- Breakdown by view type
- HTML page views: 2979
- PDF downloads: 643