Research Article Open Access
Oral Health Related Quality of Life of Patients with Disability Attending a Public Physiotherapy Clinic in Lagos, Nigeria
Oyapero A1*, Edomwonyi A1 and Akinola TO21Department of Preventive Dentistry, Lagos State University Teaching Hospital, Ikeja, Lagos, Nigeria
2Department of Physiotherapy, Lagos State University Teaching Hospital, Ikeja, Lagos, Nigeria
- *Corresponding Author:
- Dr. Oyapero A
Department of Preventive Dentistry
Lagos State University Teaching Hospital
Ikeja, Lagos, Nigeria
Tel: +234-1-8777845
E-mail: fola_ba@yahoo.com
Received Date: July 06, 2015; Accepted Date: July 23, 2015; Published Date: July 31, 2015
Citation: Oyapero A , Edomwonyi A, Akinola TO (2015) Oral Health Related Quality of Life of Patients with Disability Attending a Public Physiotherapy Clinic in Lagos, Nigeria. J Oral Hyg Health 3:182. doi: 10.4172/2332-0702.1000182
Copyright: © 2015 Oyapero A, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Visit for more related articles at Journal of Oral Hygiene & Health
Abstract
Oral health is a state of the oral and related tissues and structures that contribute positively to physical, mental and social well-being by allowing the individual to speak, eat and socialize unhindered by pain, discomfort or embarrassment. The achievement of optimum oral health can however be limited by certain disabilities. Oral diseases can also have an impact on quality of life, affecting chewing, eating, speaking, self-esteem, social interactions and relationships. The aim of this study was to determine the OHRQOL of physically challenged patients attending the physiotherapy clinic at the Lagos State University Teaching Hospital, Ikeja (LASUTH) using the Oral Health Impact Profile -14 (OHIP-14).
This cross-sectional study was conducted at the physiotherapy clinic of LASUTH. A simple random sampling technique was utilized to recruit the respondents and an interviewer administered questionnaire was employed to obtain socio-demographic information, clinical status, OHRQOL and to record the findings of the oral examination by trained examiners. Sixteen (20%) of the subjects attended the physiotherapy clinic due to a cerebrovascular accident (CVA), 14 (17.5%) had lumbar spondylitis while 10 (12.5%) had cervical spondylitis. The highest mean OHIP-14 impact score (1.67) was observed in the subdomain of discomfort on chewing. There was a strong association between the total OHIP-14 scores of the subjects and their clinical indicators.
Using the overall mean OHIP-14 scores, the educational level and the nature of disability of the subjects was significantly associated with OHRQOL with patients with CVA reporting the highest impact. Improving the levels of oral health in those with impairments or disabilities is a major issue for the dental care services. The physiotherapy clinic can be an avenue for aggressive oral health promotion activities in this group of patients.
Keywords
Disability; Oral health related quality of life; Oral Health Impact Profile-14 (OHIP-14)
Introduction
Oral health is a state of the oral and related tissues and structures that contribute positively to physical, mental and social well-being and the enjoyment of life’s possibilities, by allowing the individual to speak, eat and socialize unhindered by pain, discomfort or embarrassment. Oral health status is closely related to Quality of life which is a multidimensional entity incorporating a cognitive and an emotional component [1]. Oral diseases can have an impact on quality of life, affecting chewing, eating, speaking, self-esteem, social interactions and personal relationships [2]. Oral health problems place an extensive burden on vulnerable populations throughout the world. The achievement of optimum oral health can also be limited by certain disabilities [3].
Disability is a functional limitation based on an impaired body. Acquired disabilities generally result from trauma, such as spinal cord and head injury and chronic diseases such as arthritis, cancer, degenerative neurologic disorders and cerebrovascular accident (CVA) [4]. The oral health and dental care of the disabled has generally been reported to be poorer than that of the general population [5]. This has a wide reaching impact since poor oral health can have a negative effect on self-esteem, quality of life and general health. For people with limitations due to disabilities, the routine practice of oral care may be a considerable challenge. This is particularly evident in patients that have disabilities that affect the hands such as CVA and arthritis.
CVA is a severe neurological condition caused by a sudden interruption of the cerebral blood flow and it requires a prompt and effective response. Epidemiologic studies have shown that cerebrovascularaccident is responsible for 0.5 to 45% of neurological admissions and it has been found to be the eighth leading cause of death in Nigeria [6,7]. Physical weakness, lack of co-ordination and the cognitive problems that can accompany a CVA may make it impossible for a person to maintain good oral hygiene on their own [8]. Limb paralysis and reduced manual dexterity may affect the stroke survivor’s ability to clean their teeth and dentures and to maintain a healthy oral condition. Oro-facial motor and sensory impairments can also lead to improper dental and denture hygiene, ultimately leading to dental and periodontal diseases [9]. Additionally, anti-hypertensive medication can cause salivary dysfunction, gingival enlargement and disturbances in taste while anticoagulants can predispose to gingival bleeding [9,10].
Correspondingly, other disabilities such as arthritis have been associated with a higher prevalence of moderate to severe chronic generalised periodontitis [11]. Both Rheumatoid-(RA) and Osteoarthritis (OA) may have a profound effect on oral health as a result of physical limitations, inflammatoryand degenerative processes and the effects of medications [12,13]. The RA and OA patient’s poor ability to maintain proper oral hygiene may result in accumulation of plaque and calculus, and significantly increases the risk of periodontal disease and dental caries. Mercado et al observed a significantly higher prevalence of periodontal disease in patients with RA [14] .
There appears to be an association between a decline in the oral health status of persons with disabilities and their Oral Health Related Quality of life (OHRQOL). An investigation into the OHRQOL in adult stroke survivors in Scotland found greater impacts in the physical function, emotional and mental health domains [15]. The relationship between the impact of disabilities on the OHRQOL of patients has however received very little attention in Nigeria. The aim of this study therefore was to determine the OHRQOL of patients attending the physiotherapy clinic at the Lagos State University Teaching Hospital, Ikeja (LASUTH).
Materials and Methods
This cross-sectional study was conducted at the Lagos State University Teaching Hospital, Ikeja, Lagos, Nigeria.
Sample size
The sample size was calculated using a formula for cross sectional studies: N=Z pq/d2. Using a prevalence value of 10% for disabilities from a Nigerian study [16], a sample size of 71 was determined. 80 subjects were however recruited for the study.
Sample selection
The subjects for the study were recruited from patients on treatment appointment at the Physiotherapy clinic of LASUTH. A simple random sampling technique was utilized to recruit the respondents. The sampling frame was the attendance register for each day and the balloting method was utilized in selecting the study subjects. A total of 80 questionnaires were administered during the study on subjects who met the informed criteria and gave their informed consent.
Description of the study population
The physiotherapy clinic of LASUTH is a specialist centre that attends to about 30 patients on its clinic days. It attends to patients in its three departments namely the surgical, medical and paediatric units. The surgical unit attends to patients with trauma and those recovering from surgery while the medical unit attends to patients with CVA and those with degenerative medical conditions. The paediatric physiotherapy section attends to children with cerebral palsy, birth defects and other neurological disorders.
Inclusion and exclusion criteria
Included in the study were patients who were 18 years old and above who were willing to give their informed consent. Respondents attending the physiotherapy clinic on account of medical conditions such as CVA and those with surgical conditions such as trauma were included in the study. Those who were unwilling to give their informed consent, paediatric patients, those with severe neurological deficits that could not respond to requests for information and edentulous patients were excluded from the study. Hypertensive patients on calcium channel blockers such as Nifedipine, Diltiazem or Amlodipine that could precipitate gingival hyperplasiaand further worsen gingival inflammation were also excluded
Data collection
A structured interviewer administered questionnaire was used for data collection. The questionnaire consisted of questions on sociodemographic items including sex, age, and level of education, as well as their dental history. The OHIP-14 [17] form was used to evaluate the impact of dental and periodontal disease on the respondents’ quality of life. Subjects were asked to rate their dental experience with appropriate responses to the OHIP-14.
OHRQOL measurement with OHIP-14
The OHIP-14 [17], a 14-question instrument that focuses on seven dimensions of impact (functional limitation, pain, psychological discomfort, physical disability, psychological disability, social disability and handicap) was used. For each of the OHIP-14 questions subjects rated how frequently they had experienced an impact in the preceding months, on a 5-point Likert scale indicating if the problem had been experienced “very often” (code 4), “fairly often” (code 3), “sometimes” (code 2), “hardly ever” (code 1), or “never” (code 0). To calculate the OHIP-14 impact scores for individual domains, the mean of the subjects’ scores was obtained to give a maximum score of 4. For individual sub-domain scores 0, 1 and 2 were classified as low impact while scores 3 and 4 were classified as high impact. In order to calculate the overall OHIP-14 total impact score for all domains, item response codes were summed to give the final scores (Maximum obtainable impact score=56). The OHIP-14 final impact scores were classified as low (0-18.9), moderate (19-37.9) and high (38-56) to describe the impact level in the study population.
Dental examination
Two trained researchers carried out all clinical oral examinations under field conditions based on the World Health Organization (WHO) criteria [18], recording the data on a prepared record sheet. All fully eruptedpermanent teethwere scored, excluding third molars. The clinical examinations were conducted by means of a hand-held artificial light, two mirrors, a dental probe and a periodontal probe. The Oral Hygiene Index- Simplified by Greene and Vermillion [19,20] clinically examined the subjects for dental caries using DMFT index by Klein et al. [19] and oral hygiene status. The level of gingival inflammation was determined using the Gingival Index of Loe and Silness [21]. Periodontal status was assessed using a specially designed lightweight CPITN probe [22] with a 0.5 mm ball tip while periodontal pockets depth was measured from the edge of the free gingiva to the bottom of the pocket using the Williams periodontal probe.
Data analysis
Data was analysed using SPSS (Statistical package for social sciences) for Windows (version 18, Chicago, IL) statistical software package. Frequency distribution tables were generated for all variables and measures of central tendency and dispersion were computed for numerical variables. Since the data were normally distributed, descriptive statistics including means, standard deviations, and percentages were used to summarize the demographic variables and health-related behavior of the study sample. The Chi square test was used to determine the level of association between variables. The Anova tests were used to compare means while the Pearson’s correlation coefficient was used to determine the level of association between the variables. A 95% confidence interval and a 5% level of significance were adopted.
Results
A total of 80 subjects who were eligible by set inclusion and exclusion criteria and who gave their informed consent at the Physiotherapy clinic of Lagos State University teaching Hospital, Ikeja, were included in the study. The study was conducted from January to May 2014. All subjects were included in the final analysis.
• Socio-demographic and diabetic characteristics of the study population.
Most of the subjects (45%) were in the 41-60 years category and there were more females (55%) enrolled in the study. Majority of participants (67.5%) were married while (50%) had tertiary education. Most of the subjects (55%) had a surgical type of disability (Table 1).
| Frequency | Percentage(%) | ||
|---|---|---|---|
| Age range | 21-40 | 24 | 30 |
| (years) | 41-60 | 36 | 45 |
| 61-above | 20 | 25 | |
| Gender | Male | 36 | 45 |
| Female | 44 | 55 | |
| Marital | Married | 54 | 67.5 |
| Status | Single | 12 | 15 |
| Widowed | 14 | 17.5 | |
| Education | None | 4 | 5 |
| Primary | 16 | 20 | |
| Secondary | 20 | 25 | |
| Tertiary | 40 | 50 | |
| Nature of Disability | Medical | 36 | 45 |
| Surgical | 44 | 55 | |
| Oral Hygiene(OHI-S) | Good | 12 | 15 |
| Fare | 36 | 45 | |
| Poor | 32 | 40 | |
| Gingivitis (GI) | Mild | 34 | 42.5 |
| Moderate | 42 | 52.5 | |
| Severe | 4 | 5 | |
| CPITN Scores | 1 | 24 | 30 |
| 2 | 38 | 47.5 | |
| 3 | 14 | 17.5 | |
| 4 | 4 | 5 | |
| Total | 80 | 100 |
Table 1: Socio-demographic and clinical characteristics of the study subjects.
• Nature of disabilities in patients at the physiotherapy clinic.
Sixteen (20%) of the subjects included in the study attended the physiotherapyclinic to cerebrovascular accident, 14 (17.5%) had lumbarspondylitis while 10 (12.5%) had cervical spondylitis. The rest had other conditions described in Figure 1.

Figure 1: Nature of disabilities in patients at the physiotherapy clinic.
• OHRQOL of the study participants.
The subjects’ OHIP-14 scores are displayed in Table 2. The highest OHRQOL scores were observed in the subdomains of discomfort on chewing, self-consciousness and embarrassment. More than 20% of the subjects reported high impacts on the quality of life in these subdomains. The highest mean impact score (1.67) was observed in the subdomain of discomfort on chewing. The subjects reported very low impacts in the sub-domain of ability to function and being irritable.
| OHIP Domains | OHIP-14 | Low Impact | High Impact | Mean OHIP-14 | ||
|---|---|---|---|---|---|---|
| Sub-domains | Band- 0, 1 and 2. | Band 3 and 4 | ImpactScore | |||
| N% | N% | |||||
| Functional limitation | Words Taste |
62 72 |
77.50 90.00 |
18 8 |
22.50 10.00 |
1.45 1.10 |
| Physical pain | Pain Discomfort |
64 56 |
80.00 70.00 |
16 24 |
20.00 30.00 |
1.55 1.67 |
| Psychological discomfort | Consciousness Tense |
58 72 |
72.50 90.00 |
22 8 |
27.50 10.00 |
1.50 1.13 |
| Physical disability | Diet Interrupt |
56 60 |
70.00 75.00 |
24 20 |
30.00 25.00 |
1.60 1.37 |
| Psychological disability | Not relaxed Embarrassed |
70 60 |
87.50 75.00 |
10 20 |
12.50 25.00 |
1.17 1.40 |
| Social disability | Irritable Job |
78 68 |
97.50 85.00 |
2 12 |
2.50 15.00 |
1.02 1.20 |
| Handicap | Life Function |
66 78 |
82.50 97.50 |
14 2 |
17.50 2.50 |
1.22 1.00 |
Table 2: OHRQOL of the study subjects.
• Association between thesocio-demographic variables of the subjects and their OHRQOL
Using the overall mean OHIP-14 scores, the educational level and the nature of disability of the subjects was significantly associated with OHRQOL. Subjects who had no education had the highest mean impact scores (32.50 ± 9.81) while subjects with medical disabilities had higher impact scores (25.22±12.60). There was no significant association between the socio-demographic variables of the subjects and their OHIP-14 in any of the other categories explored. Females had higher mean impact scores (19.68±11.99) while single subjects had the least impact score (15.71 ± 11.37) (Table 3).
| Variable | N | % | Low impact | ModerateImpact | High Impact | Total Mean OHIP-14 Impact Score | |||
|---|---|---|---|---|---|---|---|---|---|
| (0- 18.9) | (19- 37.9) | (38- 56) | |||||||
| N | % | N | % | N | % | ||||
| Age category | |||||||||
| 21-40 | 24 | 30 | 14 | 17.5 | 8 | 10 | 2 | 2.5 | 16.0 ± 11.47 |
| 41-60 | 36 | 45 | 22 | 27.5 | 10 | 12.5 | 4 | 5 | 19.1 ± 11.3 |
| 61 and above | 20 | 25 | 12 | 15 | 6 | 7.5 | 2 | 2.5 | 19.9 ± 13.0 |
| χ2= 0.27df=8p= 0.99F =0.73 p= 0.48 | |||||||||
| Gender | |||||||||
| Male | 36 | 45 | 26 | 32.5 | 6 | 7.5 | 4 | 5 | 16.83 ± 11.41 |
| Female | 44 | 55 | 22 | 27.5 | 18 | 22.5 | 4 | 5 | 19.68 ± 11.99 |
| χ2= 5.58df =5p=0.06F= 1.16p= 0.28 | |||||||||
| Marital Status | |||||||||
| Single | 12 | 15 | 8 | 10 | 2 | 2.5 | 2 | 2.5 | 17.16 ± 11.65 |
| Married | 54 | 67.5 | 32 | 40 | 16 | 20 | 6 | 7.5 | 19.37 ± 11.98 |
| Widowed | 14 | 17.5 | 8 | 10 | 6 | 7.5 | 0 | 0 | 19.71 ± 11.37 |
| χ2= 3.59df= 8p= 0.46F= 0.67p= 0.55 | |||||||||
| Education | |||||||||
| None | 4 | 5 | 0 | 0 | 2 | 2.5 | 2 | 2.5 | 32.50 ± 9.81 |
| Primary | 16 | 20 | 8 | 10 | 8 | 10 | 0 | 0 | 19.87 ± 11.58 |
| Secondary | 20 | 25 | 10 | 12.5 | 6 | 7.5 | 4 | 5 | 20.80 ± 13.57 |
| Tertiary | 40 | 50 | 30 | 37.5 | 8 | 10 | 2 | 2.5 | 15.20 ± 9.87 |
| χ2= 19.50df= 11p= 0.00F= 3.57p= 0.01 | |||||||||
| Nature of Disability | |||||||||
| Medical | 36 | 45 | 14 | 17.5 | 14 | 17.5 | 8 | 10 | 25.22 ± 12.60 |
| Surgical | 44 | 55 | 34 | 42.5 | 10 | 12.5 | 0 | 0 | 12.81 ± 7.39 |
| χ2= 16.36df= 5p= 0.00F=30.01p= 0.00 | |||||||||
| Total | 80 | 100 | 48 | 60 | 24 | 30 | 8 | 10 | 18.4 ± 11.78 |
χ2- Chi Square* - SignificantF- Anova
Table 3: Association between the socio-demographic variables of the subjects and their OHRQOL.
• Association between the clinical status of the subjects and their OHRQOL
Study subjects that had cerebrovascular accident had the highest mean overall OHIP-14 impact scores [30]. They also had the highest DMFT, OHI-S and GI sores. The lowest impact scores on OHRQOL was recorded by subjects with lumbar disc herniation [7] while the lowest DMFT, OHI-S and GI sores was recorded in subjects with left shoulder dislocation (Table 4).
| Diagnosis | N | % | Mean OHIP-14 ImpactScore | Mean DMFT | Mean OHI | Mean GI |
|---|---|---|---|---|---|---|
| Medical Conditions | ||||||
| Cerebro-vascular Accident | 16 | 20.0 | 30 ± 12.89 | 2.87 ± 4.08 | 4.14 ± 1.13 | 2.03 ± 0.41 |
| Osteoarthritis | 8 | 10.0 | 18.75 ± 6.56 | 2.75 ± 3.32 | 4.01 ± 1.74 | 2.0 ± 1.01 |
| Facial palsy | 8 | 10.0 | 30 ± 8.71 | 0.00 | 3.50 ± 1.14 | 1.17 ± 0.12 |
| Rheumatoid arthritis | 4 | 5.0 | 17.00 ± 5.77 | 2.50 ± 2.77 | 3.48 ± 0.67 | 1.25 ± 0.57 |
| Surgical Conditions | ||||||
| Fracture legs | 4 | 5.0 | 14 ± 0.23 | 2.00 ± 2.30 | 1.50 ± 2.30 | 1.56 ± 0.65 |
| Fracturedhand | 4 | 5.0 | 7.00 ± 8.08 | 0.00 | 2.60 ± 0.84 | 1.50 ± 0.28 |
| L shoulder dislocation | 2 | 2.5 | 15.00 ± 0.12 | 0.00 | 1.00 ± 0.00 | 0.95 ± 0.10 |
| Lumbar metastasis | 1 | 1.25 | 17.00 ± 0.00 | 0.00 | 4.03 ± 0.00 | 1.50 ± 0.00 |
| Lumber spondylitis | 14 | 17.5 | 11.00 ± 7.31 | 1.0 ± 1.35 | 2.75 ± 1.61 | 1.0 ± 0.10 |
| Lumbar disc herniation | 2 | 2.50 | 3.00 ± 2.23 | 0.00 | 0.67 ± 0.10 | 1.17 ± 0.02 |
| Brain tumor | 1 | 1.25 | 24.00 ± 0.00 | 0.00 | 2.87 ± 0.00 | 1.87 ± 0.00 |
| Cervical fracture | 2 | 2.50 | 17.00 ± 0.12 | 0.00 | 2.50 ± 0.20 | 1.50 ± 0.15 |
| Cervical spondylitis | 10 | 12.50 | 8.5 ± 7.80 | 0.25 ± 0.46 | 1.79 ± 0.32 | 1.01 ± 0.11 |
| Rightfinger amputation | 1 | 1.25 | 19.00 ± 0.00 | 0.00 | 2.00 ± 0.00 | 1.00 ± 0.00 |
| Righthand contracture | 3 | 3.75 | 14.00 ± 0.34 | 0.00 | 1.95 ± 0.02 | 1.0 ± 0.11 |
| Total | 80 | 100 | 18.40 ± 11.78 | 1.40 ± 2.83 | 3.00 ± 1.51 | 1.47 ± 0.51 |
Table 4: Association between the clinical status of the subjects and their OHRQOL
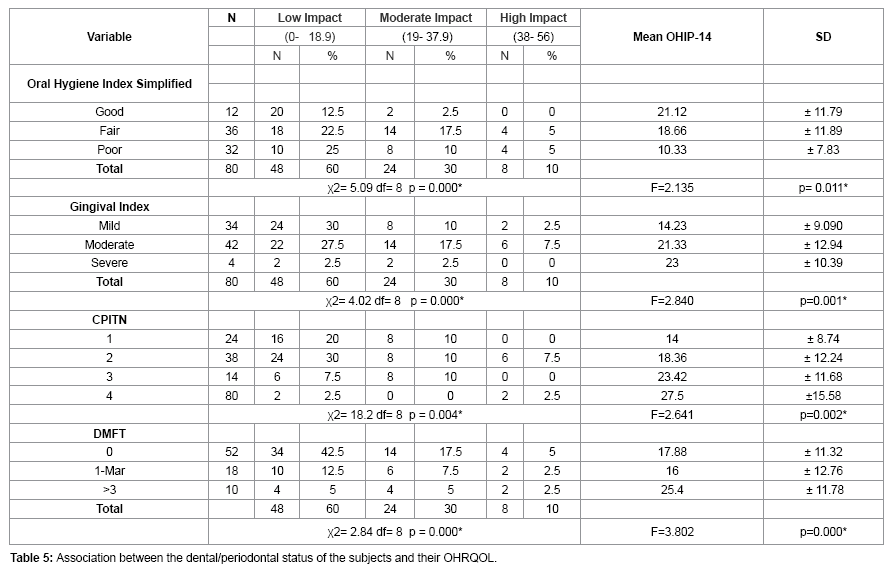
• Association between the dental/periodontal status of the subjects and their OHRQOL
Subjects with poor oral hygiene had the highest overall mean OHIP- 14 impact scores (21.12). (p=0.011). There was similarly a significant association between the gingival index of subjects and OHIP-14 (p=0.001); CPITN scores (p=0.002) and their DMFT (p=0.000). The highest overall mean OHIP scores were observed in subjects with severe gingival inflammation; deep pockets and high DMFT scores (Table 5).
Discussion
This study investigated the OHRQOL of a group of patients attending the physiotherapy clinic at the Lagos State University Teaching Hospital, Ikeja (LASUTH). Majority of subjects in this sample were female and there was a preponderance of middle aged and elderly subjects. Most of the subjects were also married and had a tertiary education. CVA, lumbar and cervical spondylitis accounted for the majority of cases seen at this clinic. Over half of the study subjects had moderate to severe gingivitis while the majority had fair or poor oral hygiene. Twenty two per cent of the subjects had CPITN scores of 3 and 4 indicating a high need for periodontal specialist treatment in this group of subjects. Marks et al. [23] similarly observed a high prevalence of gingivitis, dental caries and dental trauma among a cohort of special need athletes. This indicates a high need for oral health education and preventive programmes in this group of challenged subjects and also a great need for oral health intervention and treatment.
The study subjects reported negative impacts on their OHRQOL in all subdomains. The most common impacts were reported in the subdomains of discomfort on chewing, diet, self-consciousness and embarrassment. Study subjects that had cerebrovascularaccident had the highest mean overall OHIP-14 impact scores. They also had the highest DMFT, OHI-S and GI scores. This was in agreement with a study by Hunter et al. [15] who observed that stroke survivors reported high impacts in the domains of discomfort, self-consciousness, speech and interruption of meals. Macmillan et al. [24] also observed that the quality of life of stroke survivors was significantly impaired regardless of their state of health at the time of their discharge from the hospital. These findings confirm that the frequently encountered oral health problems in stroke survivors such as aesthetic problems, speech impairment, eating and swallowing difficulties are associated with a poor OHRQOL.
The present study demonstrated a strong association between the oral health status of the subjects and their OHRQOL. The highest overall mean OHIP-14 scores were observed in subjects with severe gingival inflammation, deep periodontal pockets and high DMFT scores. Some researchers have observed that poor oral health and impaired oral functions can lead to poor self-esteem, social isolation and depression[25]. The mouth plays important roles in appearance, speech and communication, and intimacy. Oral diseases can have an impact on the quality of life, affecting chewing, eating, speaking, selfesteem, health, social interactions and relationships. The study subjects also experienced more impacts on their quality of life with increasing age and this association was statistically significant. These findings are not surprising, since periodontal status has been observed to decline with increasing age. There is also a cumulative effect of other dental conditions. Some researchers [26] have shown that poor oral health has a negative impact on daily life for a substantial proportion of older people. These negative impacts have been shown to be particularly evident among elderly individuals who do not use dental services on a regular basis [26]
In the present study, females were also observed to report more impacts on their OHRQOL than males. One possible explanation for this tendency is that women care more about their health and their appearance and have greater aesthetic concerns than men. Females are also more expressive in describing the medical symptoms they feel and this could explain the higher impact scores recorded by them. The educational status of the subject was likewise significantly associated with OHRQOL confirming the findings of some researchers who reported that individuals with higher education reported better OHRQOL [27,28]. Level of education is an important marker of socioeconomic position and a higher education level is predictive of higher income and socio-economic status. Poorly educated patients with disability may thus be at increased risk for poor oral health.
Oral health care for adults with disabilities is a health care area that has received inadequate attention. It is estimated that one out of two persons with a significant disability cannot find a professional resource to provide appropriate and necessary dental care [29]. Preventive oral health protocols should be implemented in patients with physical, sensory or cognitive deficits that cause loss of independent oral care [30,31]. The Oral care system designed by SUMI et al. [32] can be recommended for and utilised by subjects with disabilities to improve their oral hygiene. Persons with physical impairments such as arthritis or quadriplegia should be encouraged to brush and floss independently by using adaptive devices such as enlarged handles, universal cuffs for hand attachment, or extension rods [33]. Individuals with limited dexterity or tremors, and the caregivers of dependent persons should be encouraged to utilise special toothbrushes such as automated (electric) toothbrushes [34,35]. Appropriate health policies should also make curative dental services accessible, affordable and acceptable to persons with disabilities.
Conclusion
Disabilities are unequivocally associated with a decline in oral health status as well as a poorer OHRQOL. This is particularly evident among challenged patients that are aged, poorly educated and those that have CVA. Improving the levels of oral health in those with impairments or disabilities should be a major concern for dental care services. Good oral health is essential for an individual to optimise his/her speech, nutritional intake, systemic health, rehabilitative outcomes and quality of life. All physically challenged patients should have an oral assessment which includes screening for obvious signs of dental disease, level of oral care and state of dental appliances [36]. The physiotherapy clinic can be an avenue for aggressive oral health promotion activities for this group of patients.
References
- Gift HC, Atchison KA (1995) Oral health, health, and health-related quality of life. Med Care 33: NS57-77.
- van der Horst, Scott & Bowes 2008 Primary Care Quick Fact Sheet www.rgpc.ca; COHS 2005
- Rose LF, Mealey B, Minsk L, Cohen DW (2002) Oral care for patients with cardiovascular disease and stroke. J Am Dent Assoc 133 Suppl: 37S-44S.
- DECOD Program (Dental Education in Care of the Disabled). Demographics of selected disabled populations. In: Rehabilitation of the dental patient with a disability. Seattle: DECOD, School of Dentistry, University of Washington; 1995.
- Vignehsa H, Soh G, Lo GL, Chellappah NK (1991) Dental health of disabled children in Singapore. See comment in PubMed Commons below A ust Dent J 36: 151-156.
- Ojini FI, Danesi MA. Pattern of neurological admissions at the Lagos University Teaching Hospital. Nig J ClinPract. 2003; 5:38-41
- World Health Organisation (WHO) Country mortality Fact Sheet 2006 Nigeria. Death and DALY estimates by cause, 2002.
- Arai K, Sumi Y, Uematsu H, Miura H. Association between dental health behaviours, mental/physical function and self-feeding ability among the elderly: a cross-sectional survey. Gerodontology2003; 20 : 78-83.
- Ship JA, Chavez EM (2000) Management of systemic diseases and chronic impairments in older adults: oral health considerations. Gen Dent 48: 555-565.
- Janket SJ, Baird AE, Chuang SK, Jones JA (2003) Meta-analysis of periodontal disease and risk of coronary heart disease and stroke. Oral Surg Oral Med Oral Pathol Oral RadiolEndod 95: 559-569.
- Ferraryi T, Calvano M, Armadai M, Echaide M, Scagneti G et al. (2014) Prevalence and microbiological profile of periodontal disease in patients with rheumatoid arthritis. J Disability Oral health15: 68.
- Fox PC (1994) The spectrum of salivary dysfunction in Sjögren’s syndrome and the resultant oral complications. In: Homma M, Sugai S, Tojo T, Miyasaka N, Akizuki M, eds. Sjögren’s syndrome: state of the art. Amsterdam: Kugler Publications 37-39.
- Sorsa S (1987) [Dental care for rheumatic patients].SuomHammaslaakarilehti 34: 656-659.
- Mercado F, Marshall RI, Klestov AC, Bartold PM (2000) Is there a relationship between rheumatoid arthritis and periodontal disease?J ClinPeriodontol 27: 267-272.
- Hunter RV , Clarkson JE, Fraser HW, MacWalter RS. (2006) A preliminary investigation into tooth care, dental attendance and oral health related quality of life in adult stroke survivors in Tayside, Scotland. Gerodontology 23: 140–48.
- Adeniyi EO. 30 years of providing answers to the challenges of special education in Nigeria: How far, how fair, special needs Education development in Nigeria. Past, Present, Future 2008; 25-26.
- Slade GD1 (1997) Derivation and validation of a short-form oral health impact profile. Community Dent Oral Epidemiol 25: 284-290.
- WHO. Oral Health Surveys, Basic Methods 4. edition. Geneva: WHO, 1997.
- LOE H, SILNESS J (1963) PERIODONTAL DISEASE IN PREGNANCY. I. PREVALENCE AND SEVERITY.OdontolScand 21: 533-551.
- Klein H, Palmer C.E, Knutson J.W. Studies on dental caries index, dental status and dental needs of elementary school children, Public Health Report (Wsh) 1988; 53: 751-765.
- GREENE JC, VERMILLION JR (1964) THE SIMPLIFIED ORAL HYGIENE INDEX.J Am Dent Assoc 68: 7-13.
- Ainamo J, Barmes D, Beagrie G, Cutress T, Martin J, et al. (1982) Development of the World Health Organization (WHO) community periodontal index of treatment needs (CPITN). Int Dent J 32: 281-291.
- Marks LAM, Fernandez C, Perlman S, Koehler B,KaschkeI. Oral Health of Special Olympics athletes in Europe and Eurasia. J Disability and oral health 2014; 15: 65
- McMillan AS, Leung KC, Pow EH, Wong MC, Li LS, et al. (2005) Oral health-related quality of life of stroke survivors on discharge from hospital after rehabilitation. J Oral Rehabil 32: 495-503.
- Karuza J, Miller WA, Lieberman D, Ledenyi L, Thines T (1992) Oral status and resident well-being in a skilled nursing facility population. Gerontologist 32: 104-112.
- Astrøm AN, Haugejorden O, Skaret E, Trovik TA, Klock KS (2006) Oral Impacts on Daily Performance in Norwegian adults: the influence of age, number of missing teeth, and socio-demographic factors. J Oral Sci 114: 115-121.
- Ekbäck G, Nodrehaug-Astrøm A, Klock K, Ordell S, Unell L (2010) Satisfaction with teeth and life-course predictors: a prospective study of a Swedish 1942 birth cohort. Eur J Oral Sci 118: 66-74.
- Tsakos G, Sheiham A, Iliffe S, Kharicha K, Harari D, et al. (2009) The impact of educational level on oral health-related quality of life in older people in London. Eur J Oral Sci 117: 286-292.
- Fenton SJ (1993) Universal access: are we ready? Spec Care Dentist 13: 94.
- Migliorati CA, Madrid C (2007) The interface between oral and systemic health: the need for more collaboration. ClinMicrobiol Infect 13 Suppl 4: 11-16.
- Katz RV, Smith BJ, Berkey DB, Guset A, O'Connor MP (2010) Defining oral neglect in institutionalized elderly: a consensus definition for the protection of vulnerable elderly people. J Am Dent Assoc 141: 433-440.
- Sumi Y, Nakajima K, Tamura T, Nagaya M, Michiwaki Y (2003) Developing an instrument to support oral care in the elderly. Gerodontology 20: 3-8.
- Sroda R, Plezia RA (1984) Oral hygiene devices for special patients. Spec Care Dentist 4: 264-266.
- Willette J, Tweedy C, Martin M, Leroux B, Holsapple C. Clinical trial of a 3-sided toothbrush in a disabled population. J Dent Res 1995; 74: 49.
- Finizio JM (1996) Power-assisted toothbrushes simplify hygiene for those who need extra help. RDH 16: 42-44.
- 2010 Best Practice Stroke Recommendations resource: www.strokebestpractices.ca
Relevant Topics
- Advanced Bleeding Gums
- Advanced Receeding Gums
- Bleeding Gums
- Children’s Oral Health
- Coronal Fracture
- Dental Anestheia and Sedation
- Dental Plaque
- Dental Radiology
- Dentistry and Diabetes
- Fluoride Treatments
- Gum Cancer
- Gum Infection
- Occlusal Splint
- Oral and Maxillofacial Pathology
- Oral Hygiene
- Oral Hygiene Blogs
- Oral Hygiene Case Reports
- Oral Hygiene Practice
- Oral Leukoplakia
- Oral Microbiome
- Oral Rehydration
- Oral Surgery Special Issue
- Orthodontistry
- Periodontal Disease Management
- Periodontistry
- Root Canal Treatment
- Tele-Dentistry
Recommended Journals
Article Tools
Article Usage
- Total views: 15862
- [From(publication date):
September-2015 - Jul 09, 2025] - Breakdown by view type
- HTML page views : 11089
- PDF downloads : 4773