Review Article Open Access
Laser Therapy for the Treatment of Onychomycosis: Best Evidence Based Practice or Not?
Nadia Dembskey and Heidi Abrahamse*
Laser Research Centre, Faculty of Health Sciences, University of Johannesburg, South Africa
- Corresponding Author:
- Heidi Abrahamse
Laser Research Centre, Faculty of Health Sciences
University of Johannesburg, P.O. Box 17011
Doornfontein, 2028, South Africa
Tel: +27 (11) 559-6550
Fax: +27 (11) 559-6884
E-mail: habrahamse@uj.ac.za
Received Date: June 30, 2016; Accepted Date: October 20, 2016; Published Date: October 24, 2016
Citation: Dembskey N, Abrahamse H (2016) Laser Therapy for the Treatment of Onychomycosis: Best Evidence Based Practice or Not?. Clin Res Foot Ankle 4:211. doi:10.4172/2329-910X.1000211
Copyright: © 2016 Dembskey N, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Visit for more related articles at Clinical Research on Foot & Ankle
Abstract
Onychomycosis is a very common condition that accounts for 50% of all nail pathologies. Currently 2–5% of the world population suffers from this disorder. It is primarily caused by dermatophytes, but the infection can also be caused by yeasts and non-dermatophyte moulds. Onychomycosis is a therapeutic challenge and recently there has been an increase in resistance to oral and topical antifungal agents, leading to 20-25% relapse and/or reinfection rate. During the past 5 years, the emergence of laser therapy has been the topic of discussion as a newer, safer modality of treatment.
Nail clippings and scrapings are the most common methods of sampling for suspected onychomycosis. The simplest method for detecting fungi is by way of 20% potassium hydroxide (KOH) preparations, but lately show insufficient sensitivity in onychomycosis – as much as 40–68%. Fungi can also be grown in culture form; however a 70% sensitivity detection failure rate is seen. Recently, histological fungal detection – in the form of Periodic Acid- Schiff (PAS) stain – has shown high sensitivity at 92% in the detection of fungal elements.
The exact mechanism of action of laser is unknown but it is believed that heat disintegrates fungal structures. One of the most appealing characteristics of laser therapy is its ability to deliver energy to the target tissue and avoid systemic side effects at the same time. In 2009 the United Kingdom (UK) Podiatry magazine Podiatry Now published a letter suggesting laser treatment was “possibly the most radical development in the treatment of onychomycosis our profession has ever seen”, although concerns were raised over the unproven efficacy and investment costs involved.
Papers have been published investigating the efficacy of lasers for the treatment of onychomycosis. Even though laser therapy provides an alternative option with rapid procedure duration, conflicting evidence is shown in a variety of papers and studies with longer follow-up periods suggest onychomycosis relapse in those treated with laser, which warrants further investigation.
Keywords
Onychomycosis; Resistance; Laser; New treatment; 1064 nm wavelength; Heat; Effectiveness; Review
Abbreviations
KOH: Potassium Hydroxide; PAS stain: Periodic Acid-Schiff Stain; ATP: Adenosine Triphosphate; UK: United Kingdom
Introduction
Onychomycosis, a chronic, specific fungal infection of the toenail, is a very common condition that accounts for 50% of all nail pathologies [1-7]. Currently 2–5% of the world population suffer from this disorder [8,9]. It is primarily caused by dermatophytes, but the infection can also be caused by yeasts and non-dermatophyte moulds [5,7,10-13]. Onychomycosis is a therapeutic challenge and recently there has been an increase in resistance to oral and topical antifungal agents, leading to 20–25% relapse and/or reinfection rate [2-4,6,9,10,14-17]. During the past 5 years, the emergence of laser therapy has been the topic of discussion as a newer, safer modality of treatment [2-4,8,9,14,18-20]. Although new research using phototherapy for onychomycosis shows promising short term results, these studies have a very small output and are poorly designed [14,19].
Method
This paper will describe the various types of onychomycosis, its causative organisms, types of microscopic investigations done and current treatment modalities used according to literature. The author will also discuss whether laser therapy is the new best evidence based treatment for onychomycosis or not.
Discussion
Although onychomycosis is not life-threatening, most patients seek treatment for cosmetic reasons or pain relief [4,19,21].
Causes of Onychomycosis
Dermatomycoses (sub-division: onychomycosis) is mainly caused by dermatophytes, yeasts and non-dermatophyte moulds [5,7,10-12,15,21].
The most common fungal agent that causes this condition is dermatophytes, which accounts for 60–80% of infections [5]. This is followed by yeasts and lastly (rarely) non-dermatophyte moulds [21].
Dermatophytes
Trichophyton rubrum
Trichophyton rubrum continues to be the most isolated causative pathogen for onychomycosis in the world [5,7,10-12,15,21].
In the Greek language Trichophyton means “plant” and “hair”, whilst rubrum denotes “red” [12].
This dermatophyte mainly targets nail keratin (Figure 1) [12].

Figure 1: Trichophyton rubrum on Sabouraud’s dextrose agar [12].
Trichophyton interdigitale
Trichophyton interdigitale (previously known as Trichophyton mentagrophytes) is the second most prevalent causative dermatophyte pathogen [5,7,12,21].
This infection originally starts in between the toes and later spreads to the nail (Figure 2) [12,21].

Figure 2: Trichophyton interdigitale on Sabouraud’s dextrose agar [12].
Epidermophyton floccosum
As with Trichophyton interdigitale, this infection starts on the skin and later spreads to the nails.
It is an ananthropophilic species that is a common cause of tinea pedis (athlete’s foot) (Figure 3) [12,21].

Figure 3: Epidermophyton floccosum on Sabouraud’s dextrose agar [12].
Although these dermatophytes are not exclusively the causative agents for onychomycosis, they are considered the most common [5,7,10-12,15,21].
Home Transmission and Virulence Factors of Dermatophytes
Onychomycosis transmission between family members most commonly occur via the bath [11,12].
The spread of onychomycosis is classified into two groups: horizontal spread between spouses and vertical spread between family members (most common) [12]. Virulence factors must be present for infection to occur [12,21].
Hair, skin and nail cytokeratin is the dermatophytes target structure for infection and degradation takes place through keratinase – targeting the structure’s complex proteins. Enzyme activity at normal body temperature and pH of the host skin creates a reservoir for the organism.
This means that the strain is only found on the person or in his home. Infection spread pathways are either direct (contact from one person to another – less common) or indirect (walking barefoot on contaminated surfaces – more common) [11].
Onychomycosis due to Yeasts and Non-Dermatophyte Moulds
Reports show an increase in onychomycosis caused by yeasts and non-dermatophyte moulds [12].
The most noticeable among these are Candida albicans , Candida parapsilosis , Candida glabrata , Candida krusei and Aspergillus fumigates [5,10,12,21].
Most often these moulds grow saprophytically due to contamination on nails with pathological changes, e.g. Psoriasis (Tables 1 and 2) [12].
| CLASSIFICATION | CLINICAL APPEARANCE | DESCRIPTION |
|---|---|---|
| Distal subungalonychomycosis (DSO) | 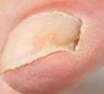 |
Distal free edge of nail Hyperkeratotic Brownish-yellow |
| Lateral and distolateralsubungalonychomycosis (DLSO) |  |
Continuation from DSO Pathogen migrates from hyponychium at side proximally Hyperkeratotic Brownish-yellow |
| Proximal subungalonychomycosis (PSO) | 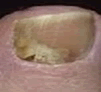 |
Rare Spreads from cuticle to eponychium in immunosuppressed patients Hyperkeratotic Brownish-yellow |
| White superficial onychomycosis (WSO) |  |
Superficial nail plate infection White plaque-like layer covers the nail plate |
| Proximal white subungalonychomycosis (PWSO) |  |
Special variant White discolouration underneath proximal part of nail plate |
| Total dystrophic onychomycosis (TDO) |  |
“Glacier nail” Longitudinal yellow streaks stretching medially and laterally reaching the nail matrix |
Table 1: Classification, clinical appearance and description of different types of onychomycosis [12,21].
| Predisposing factors |
| Diabetes Mellitus |
| Peripheral vascular arterial disease |
| Chronic venous insufficiency |
| Polyneuropathies |
| Immunosuppression |
| Microtrauma (in athletes) |
| Hyperhidrosis |
| Lymphoedema |
| Malalignment of the feet |
| Psoriasis |
| Ichthyosis vulgaris |
Table 2: Most common predisposing factors for onychomycosis [5,14].
Impaired Quality of Life and Stigmatisation due to Onychomycosis
Studies have found that generally patients with onychomycosis avoid social gatherings as they have a fear of transmitting the infection to other people [5,11,12].
When patients were asked how they feel about the stigma onychomycosis has caused, patients felt greatest impairment due to onychomycosis being contagious; felt other people would stare at their nails and felt unattractive [5,12]. The most common problems affecting patient quality of life is cutting nails; disfigurement (cosmetically); illfitting shoes, leading to pain and discomfort [5,12].
Diagnostic Sampling and Microscopic Preparations
Nail clippings and scrapings are the most common methods of sampling for suspected onychomycosis [10-12]. Research shows different microorganism detection techniques with varying sensitivity and specificity rates [5,13,21]. The simplest method for detecting fungi is by way of 20% potassium hydroxide (KOH) preparations [5,21]. Nail scrapings are taken from the infected site and mounted on a glass slide with a 20% KOH solution.
The solution is then heated to a point where the epidermal cell keratin is dissolved and the fungal elements are left. The preparation is then examined microscopically for hyphae, budding cells or spores [22]. Unfortunately the conventional KOH preparations lately show insufficient sensitivity in onychomycosis – as much as 40–68% [21].
Fungi can also be grown in culture form, using Sabouraud 2% dextrose agar, however a 70% sensitivity detection failure rate is seen, possibly due to pre-treatment with oral or topical antifungal agents [7,13]. As a result, fungi are already inhibited in vivo, preventing growth in vitro [5,21]. The presence of non-dermatophytes in the culture specimens can further confound the identification of the causal organism [22]. Recently, histological fungal detection – in the form of Periodic Acid-Schiff (PAS) stain – has shown high sensitivity at 92% in the detection of fungal elements [13,14,21]. In this method the fungal wall glycoprotein, basement membrane material and mucosubstances are stained bright red, whilst other background elements are stained pink-blue [22,23]. However, specificity is low as there is no indication of fungal genus of species [21]. When it comes to histological PAS staining, it is imperative that nail evaluations be done by a histopathologist, so as to avoid incorrect diagnoses, e.g. nail dystrophy, Psoriasis, etc. [14,21,23].
Current Treatment Modalities for Onychomycosis
Oral antifungal agents (terbinafine hydrochloride, itraconazole and fluconazole) are the medications of choice for this condition, as either continuous or “pulse” therapies [7,10,13]. Terbinafine hydrochloride is still considered the gold standard first-line treatment. However, it is contraindicated in certain patient groups, including those with any variant of liver impairment or disease [24].
Recently there has been an increase in resistance shown to these medications – oral terbinafine hydrochloride with an efficacy of 35– 78% and itraconazole being even less effective [24,25] and various questions remain as to their safety for patients and their potential to cause hepatotoxicity and drug interactions [3,4,9,10,15-17,22,24,25].
Topical antifungal treatments in the form of nail lacquers (amorolfine and ciclosporox) are preferred by most patients as they have less serious side effects.
These agents can only be administered to those who have onychomycosis without matrix involvement and requires extensive patient monitoring, as lacquers need to be applied weekly for a period between nine to twelve months [9,22,24].
Serious questions also arise on the effectiveness of nail penetration as well as issues relating to increased organism resistance [1,9,10,15]. Despite diligent patient application, ciclosporox is only effective in about 10% of patients [24].
New Emerging Laser Therapy for the Treatment of Onychomycosis
Limitations in outcomes of both oral and topical antifungal agents have led to the investigation of laser and light as a possible new way of treating onychomycosis [3,8,18].
This new treatment modality has only been in the spotlight since 2010, although scientists have been looking into laser therapy as early as 1980 [14].
Mechanism of Action
Laser is an acronym for “light amplification by stimulated emission of radiation”. They can be spot focused while maintaining a very high radiance [22].
The exact mechanism of action of laser is unknown but it is believed that heat disintegrates fungal structures. Studies show lasers of nearinfrared light range with wavelengths of 780–3000 nm being used, but most commonly the Nd: YAG 1064 nm laser [8,13].
The 1064 nm wavelength has the ability to pass into the nail bed. Consequently, any fungal material in the nail bed is heated to extremely high temperatures which inhibits growth, causes damage and targets cells. With the high temperatures, toxic levels of adenosine triphosphate (ATP) and oxygen are created, disrupting fungal mitochondrial membrane potential, leading to slower growth rates and eventually growth completely stops [8,13,14,25].
It is also suggested that the 1064 nm might be useful in targeting the blood supply associated with fungal viability as this wavelength is readily absorbed by Haemoglobin [25].
However, heat should exceed 45°C as normal body temperature (37°C) is the optimal growth temperature for fungi [8,13,14].
Clinical Method of Laser Application
After establishing microscopic evidence of onychomycosis, photos of infected nails are taken to determine new nail regrowth after an extended period of time – usually between two and 16 weeks [2,8,25].
All patients receiving laser therapy undergo routine general podiatric care (thinning of hypertrophic and onycholytic nail plate to the thickness of 1-3 mm) prior to the procedure. No intravenous or topical anaesthetic is given [25].
Spot diameters, energy fluence and exposure time all vary, but are applied in a criss-cross pattern (vertically and horizontally) with two alternating passes of laser pulses to cover the full nail surface [2,3,4,8,13,25].
Nail plate temperature may be taken immediately after the procedure to establish efficacy of treatment [8]. No home treatment is required by the patient after the laser procedure, however more than one treatment may be necessary (Figure 4) [3,8,25].

Figure 4: Patient X’s nail prior and post 9 months treatment [25].
Review of Lasers for the Treatment of Onychomycosis: Evidence Based or Not?
One of the most appealing characteristics of laser therapy is its ability to deliver energy to the target tissue and avoid systemic side effects at the same time [24]. In 2009 the United Kingdom (UK) Podiatry magazine Podiatry Now published a letter suggesting laser treatment was “possibly the most radical development in the treatment of onychomycosis our profession has ever seen”, although concerns were raised over the unproven efficacy and investment costs involved [14]. Recently preliminary studies show good clinical and microscopical cure rates using the 1064 nm laser in the short term [2,4,11,18,20].
In Vitro Studies
One study achieved 100% inactivation of Trichophyton rubrum in vitro 91 h after treatment with an 870/930 nm dual wavelength laser, using a 1.5 cm diameter flat-top projection with a power density of 5.66 W cm-2. The same projections were used on Candida albicans at physiologic temperatures and these fungi were completely inactivated at just 20 h. Notably an increase in reactive oxygen species and a decrease in transmembrane potentials of fungi were measured using non-lethal dosimetry. Afterward, human pilot studies were performed and no damage to nail matrix was observed [26]. Another study conducted by Manevitch et al. took nail clippings infected with Trichophyton rubrum and irradiated it with an 870 nm infrared titanium sapphire laser. Intensities of 7 × 1031 photons/m2s were used and as a result negative cultures were produced 4 weeks postirradiation [24].
Vural et al. treated Trichophyton rubrum colonies with various lasers ranging from 585 nm pulsed dye to 2940 nm Er: YAG and discovered that they did not inhibit fungal growth, however, colonies treated with Q-switched 532 nm and 1064 nm Nd: YAG lasers had a significantly lower growth rate [27]. They noted that the efficacy of the 532 nm wavelength may be related to the absorption of the red pigment xanthomegnin, which is present in Trichophyton rubrum (red hairy plant) (Table 3) [27].
| AUTHORS | ORGANISM | LASER | POWER DENSITY | OUTCOMES |
|---|---|---|---|---|
| Bornstein et al. | Trichophytonrubrum | 870/930 nm dual wavelength | 5, 66 W cm-2 | 100% inactivation after 91 h |
| Candida albicans | 870/930 nm dual wavelength | 5, 66 W cm-2 | 100% inactivation after 20 h | |
| Becker and Bershow | Trichophytonrubrum | 870 nm infrared titanium sapphire | 7 �? 1031 photons/m2s | Negative culture 4 weeks post irradiation |
| Vural et al. | Trichophytonrubrum | 585 nm pulsed dye to 2940 nm Er: YAG | Did not inhibit fungal growth | |
| Trichophytonrubrum | Q-switched 532 nm and 1064 nm Nd: YAG | Colonies had significantly lower growth rates |
Table 3: Summary of results obtained for in vitro studies [24,26,27].
In Vivo Studies
Horine et al. yielded retrospective results from an international multicentre study of 262 patients. Patients received one PinPointe short-pulsed Nd: YAG 1064 nm laser treatment. A single spot consisted of a pulse train of ten 200 mJ, 90 μs duration pulses at 1064 nm, delivered into a 1.5 mm spot. Laser was delivered in a 1.0-1.5 mm spacing grid pattern. The average light dose per nail plate was 115 J/ cm2. One or two laser passes was delivered per infected nail. Pretreatment debridement and thinning of onycholytic hyperkeratotic nail plate to 1 mm was achieved using a high-speed burr. Photographs were taken of the hallux at baseline and at post-procedure follow-up. A 100% response rate was seen with a mean of 78% absolute clear nail was achieved at seven month post-procedure follow-up [25].
Becker and Bershow reviewed three studies which achieved clinical success using a 1064 nm Nd: YAG laser. One study 72 patients received four laser treatments with one week between sessions. Three months post-treatment, 95.8% were clinically clear and culture negative. No details on culture sampling or laser parameters was given. All patients were followed up 6, 9 and 12 months post-procedure for recurrence and at the end of the study all patients were clinically and culture negative. In the second study eight patients were treated every three weeks for three sessions with a 1064 nm pulsed Nd: YAG laser. Seven out of eight patients were culture negative after the third treatment. No significant side effects were reported. These patients were also prescribed a topical nail lacquer after the first laser treatment. A third study conducted by Kimura et al. irradiated 37 toenails with microscopically confirmed onychomycosis up to three times with a 1064 nm Nd: YAG laser. At 16 weeks post-procedure follow-up 81% of toenails exhibited moderate to complete clearance [2,24].In 2014, Birstow did a systematic review of the effectiveness of lasers in the treatment of onychomycosis. Any original study, published in a peer reviewed journal, which examined the use of a laser technology in the treatment of onychomycosis was considered for inclusion. The initial search yielded 268 potential papers. Subsequently, duplicate papers, papers that did not fit the inclusion criteria and papers whose full study details were not obtainable were excluded from the review.
The remaining 12 papers that were published in the last four years were included in the review. He concluded that to date the data reported was at a low level of evidence as it was made up predominantly of case series involving a small number of patients with only two small randomised controlled studies (Table 4) [14].
| AUTHORS | LASER | PATIENTS/NAILS | TREATMENT DURATION | OUTCOMES |
|---|---|---|---|---|
| Horineet al. | PinPointe short-pulsed 1064 nm Nd: YAG | 262 patients | One treatment per infected nail | 100% response rate; mean of 78% absolute clear nail at 7/12 follow up |
| Becker and Bershow | 1064 nm Nd: YAG | 72 patients | Four treatments; one week between sessions | 95, 8% clinically clear and culture negative at 3/12 follow up |
| 1064 nm Nd: YAG | 8 patients | Every three weeks for three sessions (3; 6; 9) | Seven out of eight patients culture negative after third treatment Note: Topical antifungal prescribed after first treatment |
|
| 1064 nm Nd: YAG | 37 toenails | Up to three treatments | 16 weeks follow up 81% exhibited moderate to complete clearance | |
| Birstow | Noveon continuous wave 830 nm/930 nm | 37 toenails (26 treated; 11 control) | One treatment per infected nail | 6/12 follow up; Complete clearance/markedly improved: 2 treated nails vs. 2 controls Slight/moderate improvement: 18 treated nails vs. 3 control Unchanged: 6 treated nails vs. 6 control |
| Q-clear Q-switched 1064 nm/532 nm Nd: YAG | 131 patients | Two treatments 30 days apart | 2/12 follow up microscopy and culture cure rate of 95, 4% | |
| 1064 nm Nd: YAG short pulse vs. long pulse | 10 patients | Two treatments four weeks apart | 9/12 follow up microscopy and culture cure rate of 65% Only 4 cases visibly improved (photo evidence) |
Table 4: Summary of results obtained for In Vivo studies [14,24,25].
Conclusion
In the last five years, papers have been published investigating the efficacy of lasers for the treatment of onychomycosis.
Even though laser therapy provides an alternative option with rapid procedure duration, virtually no side effects, no blood monitoring and few contraindications, conflicting evidence is shown in a variety of papers, study designs are poor with small study samples, limited output with no clear protocol and studies with longer follow-up periods suggest onychomycosis relapse in those treated with laser, which warrants further investigation.
To date, oral terbinafine hydrochloride has a high cure rate five years post-treatment at 46% and is still considered the most effective, proven, long-term treatment for onychomycosis in patients without contraindications to oral antifungal therapy.
Ethics Approval and Consent to Participate
As this is a review article on studies previously conducted, ethical approval and consent to participate was obtained prior to publication.
Availability of Data and Materials
The data contained herein is available as referenced.
Competing Interests
The authors declare that they have no competing interests.
Acknowledgement
This review was conducted at the Laser Research Centre at the University of Johannesburg and was supported by the National Laser Centre of South Africa.
Financial Supporters
Laser Research Centre, National Laser Centre (CSIR), South African Research Chair Initiative (SARChI), National Research Foundation (NRF).
References
- Baran R, Kaoukhov A (2005) Topical antifungal drugs for the treatment of onychomycosis: An overview of current strategies for monotherapy and combination therapy. J EurAcadDermatolVenereol 19: 21-29.
- Kimura U, Takeuchi K, Kinoshita A, Takamori K,Hiruma M, et al. (2012)Treating onychomycoses of the toenail: Clinical efficacy of the sub-millisecond 1064 nm Nd: YAG laser using a 5 mm spot diameter. J Drugs Dermatol 11: 496-504.
- Ortiz AE, Avram MM, Wanner MA (2014) A review of lasers and light for the treatment of onychomycosis. Lasers Surg Med46: 117-24.
- Suga Y, Kimura U, Hiruma M (2014) Can persistent toenail fungus be successfully treated with laser? Med Mycol J55:65-71.
- Tchernev G, Penev PK, Nenoff P, Zisova LG, Cardoso JC, et al. (2013)Onychomycosis: Modern diagnostic and treatment approaches.Wien Med Wochenschr 163:1-12.
- Tosti A (2013)Efinaconazole solution 10%:Topical antifungal therapy for toenail onychomycosis. Cutis92: 203-208.
- Welsh O, Vera-Cabrera L, Welsh E (2010)Onychomycosis. ClinDermatol28: 151-159.
- Nenoff P, Grunewald S, Paasch U (2014) Laser therapy of onychomycosis. J DtschDermatolGes 12: 33-38.
- Waibel J, Wulkan AJ, Rudnick A (2013) Prospective efficacy and safety evaluation of laser treatments with real-time temperature feedback for fungal onychomycosis. J Drugs Dermatol12: 1237-1242.
- Evans EG (1998) Causative pathogens in onychomycosis and the possibility of treatment resistance: A review. J Am AcadDermatol38: S32-S36.
- Gupta AK, Paquet M, Simpson FC (2013) Therapies for the treatment of onychomycosis. ClinDermatol 31: 544-554.
- Nenoff P, Krűger C, Ginter-Hanselmayer G, Tietz HJ (2014) Mycology –An update. Part 1: Dermatomycoses:Causative agents, epidemiology and pathogenesis. J DtschDermatolGes12:188-210.
- Noguchi H, Miyata K, Sugita T, Hiruma M, Hiruma M (2013) Treatment of onychomycosis using a 1064 nm Nd. YAG laser. Med Mycol J 54:333-339.
- Bristow IR (2014) The effectiveness of lasers in the treatment of onychomycosis: A systemic review. J Foot Ankle Res7: 1-10.
- Evans EG (1999) Resistance of Candida species to antifungal agents used in the treatment of onychomycosis: A review of current problems.Br J Dermatol 141: 33-35.
- Gupta AK, Simpson FC (2012) New therapeutic options for onychomycosis. Expert OpinPharmacother13: 1131-1142.
- SigurgeirssonB, Olafsson JH, Steinsson JT, Kerrouche N, Sidou F (2010) Efficacy of amorolfine nail lacquer for the prophylaxis of onychomycosis over 3 years. J EurAcadDermatolVenereol24: 910-915.
- Bunert N, Homey B, Gerber PA (2013) Onychomycosis. Successful treatment with a 1064nm Nd. YAG laser. Hautarzt64: 716-718.
- Gupta AK, Paquet M (2015) A retrospective chart review of the clinical efficacy of Nd. YAG 1064nm laser for toenail onychomycosis. J Dermatolog Treat 26: 376-378.
- Heers H, Jäger MW, Raulin C (2014) Treatment of onychomycosis using the 1064 nm Nd. YAG laser: A clinical pilot study. J DtschDermatolGes12: 322-329.
- Nenoff P, Krüger C, Schaller J, Ginter-Hanselmayer G, Schulte-Beerbühl R, et al. (2014) Mycology – An update Part 2: Dermatomycoses: Clinical picture and diagnosis. J DtschDermatolGes 12: 749-777.
- Glaser HJ, Lockwood C, Lisy K (2015) The effectiveness of laser treatments for onychomycosis in adults in the community: A systemic review protocol. J Foot Ankle Res 8: 1-15.
- Shemer A, Davidovici B, Grunwald MH, Lyakhovitsky A, Amichai B (2012)Onychomycosis: A simpler in-office technique for sampling specimens. J FamPrac 61: 552-554.
- Becker C, Bershow A (2013) Lasers and photodynamic therapy in the treatment of onychomycosis: A review of the literature. Dermatology Online 19: 1-5.
- Horine C, Dow H, Cozzarelli J (2012) Evaluation of a short pulse Nd. YAG laser procedure for infected nails: A retrospective international multicentre study of 262 patients. Cynosure 921-0406-000 Rev 110/12.
- Bornstein E, Hermans W, Gridley S, Manni J (2009) Near-infrared photoinactivation of bacteria and fungi at physiologic temperatures.PhotochemPhotobiol86:1364-1374.
- Vural E, Winfield HL, Shingleton AW, Horn TD, Shafirstein G (2008) The effects of laser irradiation in Trichophytonrubrum growth. Lasers M ed Sci23:349-353.
Relevant Topics
Recommended Journals
Article Tools
Article Usage
- Total views: 17020
- [From(publication date):
November-2016 - Jul 01, 2025] - Breakdown by view type
- HTML page views : 15949
- PDF downloads : 1071