Case Report Open Access
High-pressure Water Jet Injury to the Abdomen: A Case Report and Literature Review
Faye Magneson2, Jamie O’Rear1*, Alyson Liew-Spilger2, Joseph Capannari2, Edward Delle Donne2, Ellen Seiffert3, Donald Zimmer2 and Mark Walsh11Indiana University School of Medicine in South Bend, Notre Dame Ave, South Bend, IN 46617, USA
2Memorial Hospital of South Bend, USA
3Geisel School of Medicine at Dartmouth, USA
- *Corresponding Author:
- Jamie O’Rear
Indiana University School of Medicine-South Bend
100 Raclin-Carmichael Hall, 1234 N Notre Dame Ave
South Bend, IN 46617, USA
Tel: 574-276-5434
E-mail: jacanter@iupui.edu
Received date: November 03, 2014; Accepted date: November 26, 2014; Published date: December 01, 2014
Citation: Magneson F, O’Rear J, Liew-Spilger A, Capannari J, Donne ED, et al. (2014) High-pressure Water Jet Injury to the Abdomen: A Case Report and Literature Review. Occup Med Health Aff 2:188. doi: 10.4172/2329-6879.1000188
Copyright: © 2014 Magneson F, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Visit for more related articles at Occupational Medicine & Health Affairs
Keywords
High-pressure water jet; High-pressure injection injury; Water gun
Abbreviations
PVC: Polyvinyl Chloride; IVC: Inferior Vena Cava; LLQ: Left Lower Quadrant; LUQ: Left Upper Quadrant; RLQ: Right Lower Quadrant; RUQ: Right Upper Quadrant; SBR: Small Bowel Resection
Introduction
The rise in high-pressure water jet injuries over the last century corresponds to the increased usage of this technology in a number of industries. Some of the most common applications include the use of water injection to stimulate oil production in reservoirs, the use of hydroblasting in industrial cleaning, and the use of water jet cutting to engrave or slice materials like sheet metal, concrete, and glass. These devices generate pressures up to 55,000 pounds per square inch (psi) and can deliver liquid at flow rates up to 60 gallons per minute [1,2]. Depending on the surface area of the nozzle, fluid velocities can mimic those of military rifles in the range of thousands of feet per second.
High-pressure water jet injuries most commonly affect the upper or lower extremities, but rarely affect the abdomen or thorax. Regardless of the affected anatomical structure, the entrance wound is typically small with minimal external tissue damage, but the external exam correlates poorly with the significant extent of internal tissue damage [1-3]. As such, these workplace injuries must be treated as surgical emergencies requiring exploration, irrigation, and repair. This article presents a rare case of penetrating abdominal injury caused by a damaged hydraulic water gun, reviews documented cases of high-pressure water jet abdominal injuries to date, and describes appropriate management following an injury.
Case Report
A 31-year old man presented to the Emergency Department several hours after being injured while using a hydraulic water gun for industrial cleaning. A jet of water sprayed from a crack in the hose, hitting his abdomen with an estimated force of 14,000 psi. The stream hit his abdomen tangentially, crossing from left to right. It struck the left side of his shirt, grazed his skin at the midline, and penetrated the abdomen in the right lower quadrant (Figures 1 and 2). His past medical history was unremarkable. On presentation, he was hemodynamically stable (BP 134/82, heart rate 53/min, respiratory rate 18/min, oxygen saturation 100% on 3L nasal cannula). Physical exam was unremarkable with the exception of his abdominal exam, revealing a penetrating wound along the suprapubic region, just to the right of the midline, measuring 2.5 cm in length surrounded by a region of subcutaneous edema measuring 5 cm in diameter. The abdomen was soft with tenderness in the right lower quadrant. No rebound tenderness was present. CT scan revealed hemopneumoperitoneum, and the patient was taken emergently to the operating room for an exploratory laparotomy.
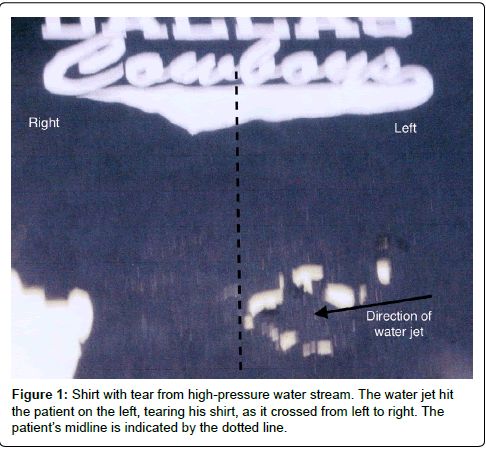
Figure 1: Shirt with tear from high-pressure water stream. The water jet hit the patient on the left, tearing his shirt, as it crossed from left to right. The patient’s midline is indicated by the dotted line.
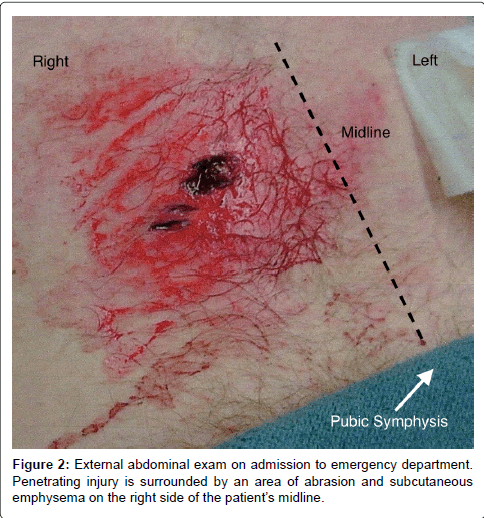
Figure 2: External abdominal exam on admission to emergency department. Penetrating injury is surrounded by an area of abrasion and subcutaneous emphysema on the right side of the patient’s midline.
A large amount of blood was evacuated from the abdominal cavity. The entire abdomen was explored, and no injury to the viscera was identified. A penetrating lesion was identified in the lower right anterior abdominal wall lateral to the rectus abdominis muscle (Figure 3). Soft tissue injury to the right retroperitoneum was identified as the source of bleeding. The absence of injury to intermediate visceral structures suggests the water stream tracked along a tissue plane, extending the injury along the abdominal wall, but avoiding the abdominal viscera.
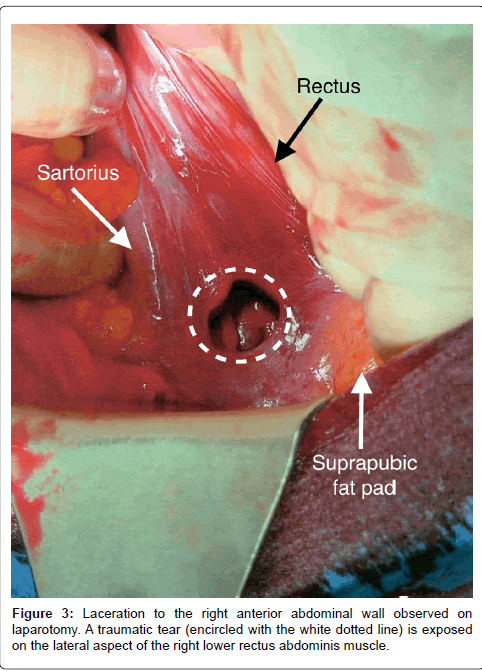
Figure 3: Laceration to the right anterior abdominal wall observed on laparotomy. A traumatic tear (encircled with the white dotted line) is exposed on the lateral aspect of the right lower rectus abdominis muscle.
No major vascular structures were damaged, and soft tissue oozing rather than a single injured vessel was identified as the source of bleeding; therefore, hemostasis was achieved by placing FloSeal Hemostatic Matrix (Baxter Healthcare, Hayward, CA) in the retroperitoneal wound. There were no surgical complications. Ampicillin-sulbactam was administered for a 24-hour period perioperatively, and no further antibiotic treatment was required. The patient had an uneventful postoperative course, and was discharged on postoperative day five after return of bowel function.
Review of Literature
There have been numerous reports of high-pressure fluid jet injuries to the upper and lower extremities since 1937 [4-6], but only ten cases of high-pressure water jet injuries to the abdomen have been reported since 1966. Details of each case are summarized in Table 1. Patients were all men ages 25-51 injured while at work. Reasons cited for injuries include one case of hose blockage, five cases of a misdirected stream or user loosing grip of the hose, one case of loose fitting equipment, one case of device malfunction, one case of user error, and one unknown cause [7-16]. The initial abdominal exam for each patient revealed a soft, non-distended abdomen, with tenderness and guarding in the area localized around the wound, unless otherwise noted in Table 1.
| Paper | Source; Protective gear; Jet Pressure |
External Wound Diameter | Surgical findings | Management |
| Gardner [7] | Salt water; PVC suit 6,000 psi |
LLQ 10 cm | Non-penetrating. No surgical exploration | Local wound care |
| Neill and George [8] | Water; none 6,000 psi |
RLQ 5 cm | Perforations of ileum and cecum | Ileocecectomy and partial SBR |
| Dabrowski [9] | Water; none 8,100 psi |
LLQ 1 cm | Liver laceration, gastric and jejunal tears | Primary repair and partial SBR |
| DeBeaux [10] | Salt water; neoprene suit 14,500 psi |
RLQ 0.25 cm | Subcutaneous edema and omental tear | Irrigation |
| Estrera, et al. [11] | Water; none 6,000 psi |
LLQ 8 cm | Multiple jejunal perforations. 1 cm IVC laceration | Jejunal resection and primary IVC repair |
| Sharma and Oswanski [12] | Water; none 10,000 psi |
RLQ 1.5 cm | Cecum perforation | Right hemicolectomy |
| Kessel, et al. [13] | Water; none Unknown |
R flank abrasion. Diffusely tender | Non-penetrating. Liver lacerations, diaphragmatic tear, colon perforation. | Debridement and primary repairs |
| Costello, et al. [14] | Waste water; rubber gear 20,000 psi |
LUQ 4 cm. Fabric at margin |
Transverse colon perforation | Primary repair |
| Wojciech, et al. [15] | Water and metal ball; none 29,000 psi |
R lumbar 8 cm. Eventerated colon | Ileal rupture. Pelvic fracture from lodged 16 mm diameter metal ball. | Ileocecectomy |
| Redmond, et al.[16] | Water; none 3,700 psi |
LUQ 1 cm. Severe pain |
Transection of pancreatic duct in tail of the pancreas | Laparoscopy with irrigation |
Table 1: Summary of reported high-pressure water jet injuries to the abdomen from 1966 to the present.
Only two of ten patients avoided abdominal visceral injuries. The first patient, described by Gardner, had a non-penetrating abdominal injury. The water jet pierced his protective polyvinyl chloride (PVC) suit, and hit the abdomen at an oblique angle, scoring the abdominal wall but failing to penetrate the abdominal cavity. The water jet stream caused edema, emphysema, and deep abrasion of the abdominal wall [7]. The second patient, described by DeBeaux, was underwater, and wearing a thick, neoprene diving suit. The stream penetrated the abdominal cavity, but caused only mesenteric bruising and an omental tear [10]. Dispersion of kinetic energy through the neoprene diving suit may have reduced the severity of internal injury.
Kessel described a patient who presented with visceral injury, despite sustaining a non-penetrating abdominal injury. Liver lacerations, a diaphragmatic tear, and perforation of the ascending colon required surgical intervention in this patient with a blast-pattern of injury [13]. All other patients sustained penetrating abdominal injuries associated with a combination of bowel perforations, pancreatic transection, or liver or vascular lacerations [8,9,11,12,14-16]. These reports highlight the potential for extensive internal injury with only minimal external damage.
Discussion
Individuals using high-pressure fluid devices must receive thorough training in the safe use of these devices and the recommended safety equipment. The most common cause of abdominal injury from one of these devices was a misdirected fluid stream from loosing grip of the hose and nozzle. While accidents may happen to workers trained in safety protocols, it is notable that the patient in this case report as well as seven of ten patients reviewed were wearing no protective gear. When injuries from high-pressure water jets do occur, appropriate management requires consideration of the anatomic injury, the chemical properties of the injected material, and the introduction of pathogens.
Anatomic injury
Kinetic energy delivered from the high velocity of a water jet is the primary determinant of tissue disruption. The water stream disperses when it strikes the skin, tracking along tissue planes, and manifesting as a small entrance wound with a wider zone of internal injury [3]. This pattern of injury is similar to that of high velocity missiles, like military and hunting rifles. Dissipating energy can also cause a blast pattern of injury where the damage is caused by pressure waves rather than direct penetrating injury [13]. In the patient presented in this case report, dispersion of energy along a tissue plane was responsible for his injuries. Energy from the water stream appeared to track along his abdominal wall, causing retroperitoneal soft tissue damage. He did not suffer from any visceral or blast pattern injuries, and this may be partially due to the fact that the stream struck his abdomen at an oblique angle, rather than perpendicular to the abdominal wall.
Though protective clothing cannot completely divert a highpressure water stream, thick materials serve as an initial barrier, absorbing some of the energy, and potentially reducing the severity of injury. The two patients reviewed who did not sustain visceral injuries were wearing either PVC protective gear or a thick neoprene diving suit [7,10]. Protective gear is highly recommended, but does not eliminate the need for immediate medical evaluation and surgical consultation in the event of an injury, regardless of a benign external exam.
Chemical irritation
Chemical irritation from the injected substance, which may include waste-water, water mixed with detergent, or sand particles for hydroblasting, can further aggravate anatomic injury, causing extensive inflammation and tissue necrosis [3,17]. It is important to identify the injected substance to direct treatment. The most serious chemical damage comes from injected solvents, like paint and paint thinners, which require debridement due to extensive tissue necrosis [3,18]. Water mixtures require irrigation, but should also be evaluated for debridement because other material can be forced into tissues with the fluid stream, like shreds of fabric from clothing or protective gear. The patient in this case report required an exploratory laparotomy with irrigation. During the laparotomy, no foreign objects or necrotic tissues were identified. The injected stream was fresh water; therefore irrigation was performed, but no debridement was necessary.
Biologic considerations
Increased susceptibility to infections by uncommon pathogens is necessary to consider in treating high-pressure water jet injuries. Extensive tissue damage and inflammation create an environment amenable for the growth of opportunistic bacteria like Acinetobacter calcoaceticus, Pseudomonas aeruginosa, and Enterobacter cloacae. These gram-negative coccobacilli commonly exist as native flora of the skin or intestines, but only cause infection in cases of extensive tissue damage or immunosuppression [14]. Another source of infection are bacteria native to waste or river water, like the gram-negative bacilli, Aeromonas hydrophila and Citrobacter freundii, which are forced into the tissues with great pressures [3].
Three of ten patients in this review suffered from infectious postoperative complications. Neill reported a postoperative wound abscess in a patient who underwent ileocecectomy 48-hours after sustaining a water jet injury, but no culture data was reported [8]. Costello reported a wastewater jet stream injury resulting in colon perforation in which the patient developed an infection on postoperative day 3, despite empiric treatment with cefoxitin. This secondgeneration cephalosporin was selected for its coverage of anaerobic bacteria likely contaminating the peritoneum after bowel perforation. Purulent drainage from the surgical incision grew Pseudomonas and Enterococcus, which were treated successfully with levofloxacin and ampicillin [14]. Wojciech reported a hydroblast and missile injury requiring ileocecectomy, in which the patient developed a retroperitoneal abscess with Citrobacter, Enterococcus, and Enterobacter on post-operative day 25 [15].
These cases emphasize the need to administer broad-spectrum antibiotics perioperatively, keeping in mind coverage for waterborne pathogens, regardless of the water source. In this case report, the patient received ampicillin-sulbactam for a 24-hour period perioperatively, which was effective in suppressing any infectious complication. Ampicillin-sulbactam has broad gram-positive and gram-negative coverage, however, resistance to this antibiotic is not uncommon. For this reason, close monitored for signs of infection during the postoperative period is necessary. If patients do go on to develop postoperative infectious complications, broad-spectrum antibiotics should be implemented until the specific bacteria responsible for the infection are identified.
Conclusion
With the increased use of high-pressure water jets across many industries, there is a corresponding increase in the incidence of injuries. There is a need for physicians to recognize the dangers of high-pressure water jet injuries in clinically stable patients with small entry wounds, because the underlying tissue damage can be life threatening. All highpressure water jet injuries should be treated as medical and surgical emergencies, evaluating patients for high-velocity penetrating injury, blast injury, chemical irritation, and infection.
References
- Harvey RL, Ashley DA, Yates L, Dalton ML, Solis MM (1996) Major vascular injury from high-pressure water jet. J Trauma 40: 165-167.
- Bolgiano EB, Vachon DA, Barish RA, Browne BJ (1990) Arterial injury from a high pressure water jet: case report J Emerg Med 8: 35-40.
- Tejero-Trujeque R (2000) High-pressure water jet injuries: a surgical emergency J Wound Care 9: 175-179.
- Rees CE (1937) Penetration of tissue by fuel oil under high-pressure from diesel engine. JAMA 109: 866-867.
- Weltmer JB Jr, Pack LL (1988) High-pressure water-gun injection injuries to the extremities. A report of six cases J Bone Joint Surg Am 70: 1221-1223.
- Hogan CJ, Ruland RT (2006) High-pressure injection injuries to the upper extremity: a review of the literature J Orthop Trauma 20: 503-511.
- Gardner AW (1966) High pressure water injury Trans SocOccup Med 16: 30.
- Neill RW, George B (1969) Penetrating intra-abdominal injury caused by high-pressure water jet Br Med J 2: 357-358.
- Dabrowski Z, Nagay B, Szacillo A (1974) [Abdominal injury caused by jet of water under pressure] Pol PrzeglChir 46: 167-168.
- De Beaux JL (1980) High-pressure water jet injury Br Med J 280: 1417-1418.
- Estrera AL, Aucar JA, Wall MJ Jr, Granchi TS, Mattox KL (1999) Hydroblast injuries to the small bowel and inferior vena cava J Trauma 47: 979-981.
- Sharma OP, Oswanski MF (2002) Hydroblast intra-abdominal organ trauma J Emerg Med 22: 49-53.
- Kessel B, Eilam D, Ashkenazi I, Alfici R (2005) Severehydroblast intra-abdominal injuries due to high-pressure water jet without penetration of abdominal cavity. Injury Extra 36: 82-83.
- Costello MW, Bolling RP, Gonzalez RP (2008) Intra-abdominal injury as a result of high-pressure water injection J Trauma 65: 222-224.
- Marks W, Białko M, Stasiak M, Deja W, Penkowski M, et al. (2009) Mixed hydroblast and missile injury with abdominal eventeration: case report BMJ Case Rep 2009.
- Redmond CE, McEvoy SH, Ryan ER, Hoti E (2013) Pancreatic transection as a result of a high-pressure water jet injury BMJ Case Rep 2013.
- Fialkov JA, Freiberg A (1991) High pressure injection injuries: an overview J Emerg Med 9: 367-371.
- Schoo MJ, Scott FA, Boswick JA Jr (1980) High-pressure injection injuries of the hand J Trauma 20: 229-238.
Relevant Topics
- Child Health Education
- Construction Safety
- Dental Health Education
- Holistic Health Education
- Industrial Hygiene
- Nursing Health Education
- Occupational and Environmental Medicine
- Occupational Dermatitis
- Occupational Disorders
- Occupational Exposures
- Occupational Medicine
- Occupational Physical Therapy
- Occupational Rehabilitation
- Occupational Standards
- Occupational Therapist Practice
- Occupational Therapy
- Occupational Therapy Devices & Market Analysis
- Occupational Toxicology
- Oral Health Education
- Paediatric Occupational Therapy
- Perinatal Mental Health
- Pleural Mesothelioma
- Recreation Therapy
- Sensory Integration Therapy
- Workplace Safety & Stress
- Workplace Safety Culture
Recommended Journals
Article Tools
Article Usage
- Total views: 22624
- [From(publication date):
December-2014 - Dec 12, 2024] - Breakdown by view type
- HTML page views : 18042
- PDF downloads : 4582