Research Article Open Access
Effect of Manual Force on Lumbar Side Bending Range of Motion
Tomonori Sato*Department of Physical Therapy, Tokoha University, 1-30 Mizuochi, Aoiku 420-0831, Japan
- *Corresponding Author:
- Tomonori Sato
Department of Physical Therapy
Tokoha University, 1-30 Mizuochi
Aoiku 420-0831, Japan
Tel: 81-54-297-3244
E-mail: tomo310@mb.infoweb.ne.jp
Received date: December 10, 2014, Accepted date: February 12, 2015, Published date: February 17, 2015
Citation: Sato T (2015) Effect of Manual Force on Lumbar Side Bending Range of Motion. Occup Med Health Aff 3:194. doi: 10.4172/2329-6879.1000194
Copyright: © 2015 Sato T. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Visit for more related articles at Occupational Medicine & Health Affairs
Abstract
Objective: We evaluated the immediate changes in intervertebral motion after application of lumbar manual force.
Methods: Fifteen male volunteers (aged 26–43 years) with no history of significant low back pain were recruited to participate as a study group (manual traction). Control group (without manual traction) consisted of fifteen male volunteers who are matched with age (age 21-45 years). Consenting volunteers were referred for three radiographs (neutral position, right side bending position prior to manual force and right side bending position after manual force). The L3/4 segment was chosen for manual force, which was performed by a single examiner. Frontal angular rotation of each lumbar spine segment and total lumbar spinal motion were measured radio graphically before and after manual force by a single investigator (radiologist). Within-group differences were assessed with the paired t test.
Results: Analysis of the pre-and post-manual force radiographs showed a significant average increase at the L3/4 segment from 4.9° to 6.4° and an improvement in the total range of motion from 17.8° to 19.5° in the study group. No significant increase was found at the L1/2, L2/3, or L4/5 segments in the study group. In the control group, there were no significant changes in all measurements.
Conclusion: These results suggest that manual force targeting the L3/4 segment results in an immediate increase in the angular motion of the L3/4 segment and improvement in total motion of the lumbar spine.
Keywords
Manual force; Range of motion; Lumbar spine
Introduction
Manual force such as Joint mobilization and manipulation has long been used for treatments of patients with mechanical spinal pain for several purposes [1-3]. One of the purposes of this treatment is to restore the segmental range of motion (ROM). Many studies have reported increased ROM or changes in mobility after manual force, [4-15] or in combination with other treatments [16-20].
In numerous studies reporting improved ROM following manual force, a cervical ROM goniometer or inclinometer was utilized to investigate changes in ROM [4-7,10,19,20]. However, these instruments usually indicate changes in the entire cervical or lumbar ROM. They do not always provide information regarding changes in the segmental ROM. Although the active ROM may be increased due to manual force, this increase may be due to motion in neighboring segments. Further, it was difficult to determine whether the segmental ROM improved from measurements of the active ROM test.
Furthermore, in several studies [6,7,20] showing an increased active ROM or changes in motion after applying manual force, posterioranterior (PA) mobilization has been used. PA mobilization is a technique involving the application of a vertical force over the spinous process of a given vertebra. It is used with the aim of reducing pain rather than improving ROM [7,21] PA mobilization may produce motion not only in the target segment but also in neighboring segments [16-28] However, no consistent motion pattern in neighboring segments caused by PA mobilization has been identified in these studies, although a consistent motion pattern may exist in the target segment.
Several studies [22-26] have described a restricted ROM during lumbar side bending at a certain level or levels in patients with low back pain. If restriction occurs due to decreased mobility of the intervertebral joint, manual force, called lumbar side bending mobilization may be effective in restoring the segmental ROM. Lumbar side bending mobilization focuses on mobilizing a specific segment using a finger block to produce a mechanical effect. To our knowledge, only our previous study has investigated segmental changes in the side bending ROM after treatment, which reported the possibility of specific effects of manual force on the lumbar segmental side bending ROM [29] However, it needs careful understanding for the result of the study due to several limitations.
The purpose of this study was to investigate immediate changes in total lumbar motion in addition to segmental ROM after manual force in asymptomatic subjects. We also compared changes in ROM between study group and control group.
Subjects and Methods
Subjects
Thirty male volunteers employed by Bizen hospital responded to an advertisement and were recruited for the present study. They are allocated at random into two groups (15 study group: mean age 33.5 ± 6.7 years, body mass index 22 ± 0.57 kg/m2; 15 control group: mean age 33.4 ± 6.8 years, body mass index 24 ± 1.24 kg/m2) . Subjects were eligible for this study if they had no history of significant low back pain and no history of lumbar surgery. Subjects were also excluded if they had a history of disease in low back such as osteoporosis. Although symptomatic patients tend to have a more restricted ROM than that of asymptomatic subjects [30], ROM in asymptomatic subjects may not have been unrestricted [22,31]. In addition, severe degenerative change in the periarticular tissue may be observed in symptomatic patients [32-34] Tarasevicius et al. reported that as osteoarthritis develops, the capsular elasticity decreases and capsular contracture increases [32]. Thus, treatments with manual force may be effective in alleviating joint degeneration and capsular contracture if degeneration is not severe. However, no change in joint mobility would occur with fibrotic capsules resistant to the force generated by treatment with manual force if degeneration is severe. Therefore, this study used asymptomatic subjects with possible restricted range of motion but who were still likely to respond to treatment. This study was approved by the Ethical Committee for Clinical Research of Bizen Hospital. All subjects were informed of the steps involved in the radiographic procedure and about the risk of radiation. All subjects provided their informed consent before the trial.
Manual force
Manual force at the L3/4 segment was performed by a single examiner 1 with more than 10 years of experience with the technique. The technique used in this study was that one of the authors learned from post graduate seminar in University of St. Augustine for Health Sciences [35]. Subjects were placed in the prone position with the lumbar spine in a neutral position and a pillow under their abdomen for support. Standing on the left side of the subjects, the examiner applied pressure from the left to the right of the L3 spinous process with the left thumb in the spot indicated by the top clip (Figure 1).
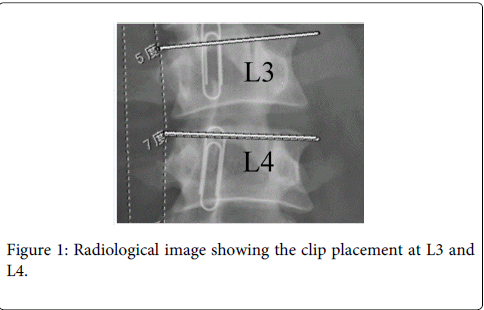
Figure 1: Radiological image showing the clip placement at L3 and L4.
Blockage of the L3 spinous process from the left to the right focused the force between L3 and L4 and minimized the amount of force above L3. The therapist placed his right hand on the medial distal thigh of the subject’s left leg. Then left lumbar side bending was introduced through left hip abduction until the therapist’s right hand felt resistance, at which point the position was held for 3 s (Figure 2).

Figure 2: Pressure from left to right of L3 for L3/4 treatment.
Instrumentation
A KXO-50G generator (TOSHIBA, Tokyo, Japan) at the setting of 320 mA was used for radiological examinations. A medium kilovoltage (average 75kV) was used. The tube was centered on L3. The focal film distance for each exposure was 100 cm.
Procedures
Subjects were placed in the prone position with their lumbar spine in a neutral position and a pillow under their abdomen for support. Subject’s upper torso was stabilized with the strap. After identification of the spinous processes of L3 and L4 via palpation, the examiner marked each by taping a paper clip to overlying skin (Figure 3). The clips placement were confirmed by radiograph, and corrected if erroneous, prior to implementing the intervention. Following, subjects were passively moved to the left side bending position through left hip abduction for the entire lumbar spine until movement of the L1/2 segment under the examiner’s left middle finger, which was positioned on the interspace between the spinous processes of L1 and L2. With the subject in this position, PA radiograph was taken. Then, subjects were randomly assigned to study group and control group. In the study group, the examiner performed manual force for L3/4 after subjects were placed in the prone position. We briefly summarize the method of manual force as we already explained. The examiner who stands on the left side of the subjects applied pressure from the left to the right of the L3 spinous process with the left thumb to minimize the amount of force above L3. Then left lumbar side bending was introduced through left hip abduction until the therapist’s right hand felt resistance. The frequency and duration of this technique was decided based on our clinical experience. Manual force was repeated three times. Three seconds of stretching was allowed each time. Then, subjects were repositioned back to the left side bending position, and postmanual force radiography was performed. In the control group, after subjects were repositioned back to the left side bending position on prone position, second radiography was performed.

Figure 3: Left lumbar side bending technique for L3/4.
The stabilizing hand (left hand) is the one providing the blocking force and the mobilizing hand (left hand) is abducting the thigh.
The segmental frontal angular rotation of each motion of the lumbar spine was measured using a modified version of previously described method of measuring sagittal angular rotation [27,28] SYNAPSE software (FUJIFILM, Stamford, CT, USA) was used for preand post-manual force radiography. Segmental frontal angular rotation was defined as the angle between the lines running through the top corners 1 through 4 (Figure 4). The total frontal angular rotation was defined and measured as the angel between the line running through the top corners of L1 and the line running through the top corners of L5. Top corners of S1 were not measured because the image of S1 is often not readily visible. Radiographic analysis was performed by a single examiner (radiologist).
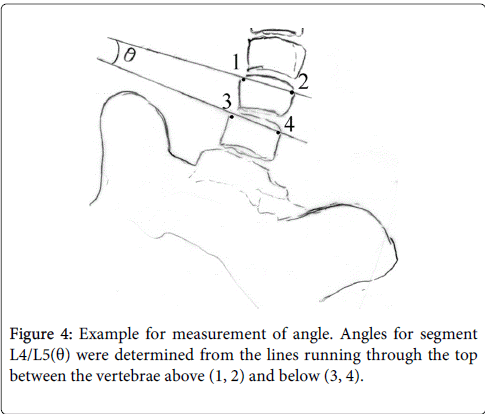
Figure 4: Example for measurement of angle. Angles for segment L4/L5(θ) were determined from the lines running through the top between the vertebrae above (1, 2) and below (3, 4).
Intra-rater reliability for radiological measurement was assessed. Second measurement was performed 24 hours later. The intraclass correlation coefficient values exceeded 0.94 (95% CI 0.81, 0.99) indicating high reliability. Furthermore, to examine variability of measurement, six subjects who have no history of low back pain were x-ray two times consecutively in side bending position and measured segmental side bending ROM at L1/2, L2/3, L3/4, L4/5. There were no significant differences in segmental side bending motion at all levels between first radiograph and second radiograph (p>0.05). Furthermore, we compared if there are any differences of side bending ROM between the study group and the control group at baseline. We confirmed that there is no significant difference of side bending ROM between the study group and the control group (L1/2: p = 0.72, L2/3: p = 0.27, L3/4: p = 0.42, L4/5: p = 0.79, Total range: p = 0.69).
Statistical analysis
Data were analyzed using the SPSS package, version 13.0 (SPSS Inc. Tokyo, Japan). The paired t-test was used to analyze differences in segmental rotation and whole lumbar side bending motion between pre- and post-manual force. Statistical significance was assumed at the 0.05 level.
Results
The values for segmental and total side bending motion with standard deviations are presented in Table 1. In the study group, differences between pre- and post-manual force radiographs demonstrated a significant improvement in L3/4 segmental motion after applying manual force (p<0.001) (Figures 5, 6 and Table 1). No significant differences in segmental motion were found at the L1/2 (p>0.05), L2/3 (p>0.05) or L4/5 (p>0.05) segment. For measurement of the total side bending range of motion, a significant increase in the range of motion was observed after manual force (Table 1). In the control group, no significant differences in segmental motion were found at the L1/2 (p>0.05), L2/3 (p>0.05), L3/4 (p>0.05) or L4/5 (p>0.05) segment between first radiograph and second radiograph. There were also no significant difference of total side bending range of motion between first radiograph and second radiograph (p>0.05).
| Level | 1st x-ray 2nd x-ray |
Means (degree) | Standard deviations (degree) | 95% confidence intervals | ||
| Lower band (degree) |
Upper band (degree) |
|||||
| L1/L2 | Study group | 1st x-ray | 3.2 | 1.1 | 2.6 | 3.8 |
| 2nd x-ray | 3.3 | 1.2 | 2.6 | 4 | ||
| Control group | 1st x-ray | 3.4 | 1.1 | 2.9 | 3.9 | |
| 2nd x-ray | 3.5 | 1.1 | 2.9 | 4.1 | ||
| L2/L3 | Study group | 1st x-ray | 4.7 | 1.8 | 3.7 | 5.6 |
| 2nd x-ray | 5 | 1.2 | 4.3 | 5.7 | ||
| Control group | 1st x-ray | 4.1 | 1.7 | 3.7 | 5 | |
| L3/L4 | Study group | 1st x-ray | 4.9 | 1.5 | 4 | 5.7 |
| 2nd x-ray | 6.4* | 1.4 | 5.6 | 7.2 | ||
| Control group | 1st x-ray | 5.6 | 1.8 | 4.6 | 5.9 | |
| 2nd x-ray | 5.4 | 1.6 | 4.5 | 6.3 | ||
| L4/L5 | Study group | 1st x-ray | 5.2 | 2.3 | 3.9 | 6.5 |
| 2nd x-ray | 5.1 | 2.3 | 3.8 | 6.4 | ||
| Control group | 1st x-ray | 4.9 | 2.1 | 4.3 | 5.8 | |
| 2nd x-ray | 4.8 | 2.1 | 3.7 | 6 | ||
| Total | Study group | 1st x-ray | 17.8 | 4.1 | 15.6 | 20.1 |
| 2nd x-ray | 19.5* | 4.1 | 17.2 | 21.7 | ||
| Control group | 1st x-ray | 17.8 | 4.1 | 16.4 | 19.4 | |
| 2nd x-ray | 18.3 | 3.5 | 16.4 | 20 | ||
| * p value < 0.001 compared with 1st x-ray (pre-manual force) NOTE. Each value represents the means and SD, 95% CI. 1st x-ray in study group: pre-manual force, 2nd x-ray in the study group: post-manual force. |
||||||
Table 1: Segmental side bending angles and total side bending angle before and after manual force.
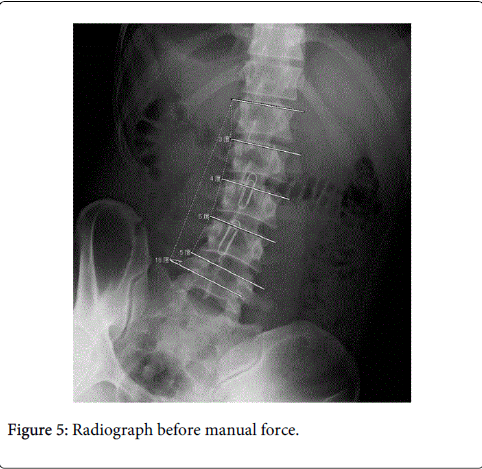
Figure 5: Radiograph before manual force.
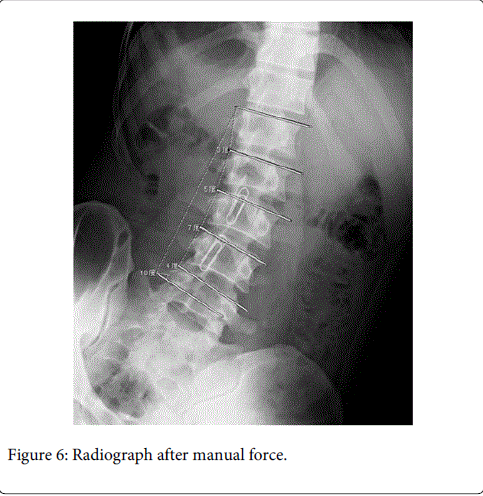
Figure 6: Radiograph after manual force.
Discussion
Although rarely reported, the technique used in this study has been applied to specific segments using the finger block technique to increase the segmental range of motion (ROM) of hypomobile segments [35]. The results of the current study may convey the idea that manual force for lumbar side bending can be used in hypomobile segments. However, to arrive at a satisfactory conclusion, subjects with hypomobile segments should be included in future studies. On the other hand, other techniques requiring manual force, such as PA mobilization, have frequently been used in previous studies [16,21] to increase motion not only in the target segment but also in neighboring segments:, thus, this technique should be considered nonspecific. Several studies16-18 have reported extension of the target segment and either flexion or extension of neighboring segments during PA mobilization. In addition, PA mobilization has often been used to reduce pain rather than improve ROM [6] The use of the finger block technique to improve ROM may have led to an increase in segmental range of motion after manual force, as used in this study. To the best of our knowledge, this is the first study to investigate the effects of a technique with manual force on the lumbar segmental side to increase ROM.
Reduced mobility in the lumbar region with pain arising from the facet joint has been previously reported [24,25,36-40] Several of these studies [37-40] using diagnostic strategies of single- and double-block facet injection techniques have identified that facet joints can be a source of low back pain. However, the relationship between pain arising from a facet joint and reduced segmental mobility has not been previously investigated. Mayer et al [24,25] reported a correlation between reduced lumbar segmental side bending mobility and pain arising from a facet joint. Thus, reduced lumbar segmental side bending mobility may be considered a common cause of pain. Moreover, previous reports have highlighted the need for physical examination and treatment of the segmental side bending to improve ROM. In accordance with the findings of these previous studies [24,25] our results indicate that this technique may be beneficial to patients with reduced segmental side bending ROM.
Our results showed improvement by 1.5° in the L3/4 segmental ROM and 1.7° in total side bending ROM following side bending mobilization. Also, other studies have demonstrated the clinical importance of reduced total lumbar side bending ROM23 and/ or reduced segmental ROM [24,25]. Furthermore, Mayer et al. [41,42] reported that improvement in inclinometric lumbar motion was correlated with decreased pain. However, no study has indicated clinically meaningful changes in total and segmental side bending ROM. Therefore, further studies are warranted to determine whether improvements of 1.5° in segmental and 1.7° in total side bending ROM following manual force have any clinical significance.
Despite the focus of manual force on the L3/4 segment in this study, a significant increase in the total ROM was observed. This result is consistent with those of previous studies in which PA mobilization caused an increase in total ROM after mobilization [6,13] As described earlier, PA mobilization causes motion at multiple levels [6-8] Thus, multiple segments must have contributed to the increase in total ROM described in these previous studies [6,13] However, in the present study, a significant increase was observed only at L3/4, as the target segment. Therefore, the improvement in total ROM was attributed to the increase in segmental ROM at L3/4. This finding differs from those of previous studies.
The subjects in the current study were asymptomatic volunteers. There are a limited number of studies that have measured segmental side bending ROM in asymptomatic subjects. Table 2 shows correlations of segmental side bending ROM with previous studies [43-46]. The average segmental motions in the current study were in accordance with previously published data of both in vivo and vitro studies. Even though most previous studies required participants to perform side bending while standing, similar range of segmental side bending motion with minor variations were shown in the current study, indicating that the method accuracy was sufficient.
| Author, year | Subjects | Mean age (range) | Method of measurement | Measurement position | Level | RSB (degree) | LSB (degree) |
| Tanz, 1953 | 14 healthy adults | (34-49) | Roentgenograms | Recumbent position | L1-2 | 2.7 | 2.7 |
| L2-3 | 3.9 | 3.9 | |||||
| L3-4 | 4 | 4 | |||||
| L4-5 | |||||||
| 4.1 | 4.1 | ||||||
| Pearcy, 1984 | 10 healthy man | 28 (22-37) | Stereoradiopgrapy | Standing | L1-L2 | 5 | 6 |
| L2-L3 | 5 | 6 | |||||
| L3-L4 | 5 | 5 | |||||
| L4-L5 | 3 | 2 | |||||
| L5-S1 | 0 | 2 | |||||
| Panjabi, 1994 | 9 fresh frozen specimes | 51 (35-62) | Stereophotogrammetry | Vertical: vertebrae was mounted | L1-L2 | 4.4 ± 0.5 | 4.0 ± 0.6 |
| L2-L3 | 5.8±1.5 | 5.8 ± 1.6 | |||||
| L3-L4 | 5.4± 1.1 | 5.1 ± 0.5 | |||||
| L4-L5 | 5.3±1.3 | 4.9 ± 0.7 | |||||
| L5-S1 | 4.7 ±0.9 | 3.9 ± 0.6 | |||||
| Steffen, 1997 | 16 healthy man | 32 (19-51) | Electromagnetic tracking system | L3-4 | 6.3 | 6.3 | |
| RSB: right side bending, LSB: left side bending | |||||||
Table 2: Segmental side bending motion in normal and cadaveric specimens from the literature.
Limitations and future study
The current study has several limitations. First, this study had only men for considering radiation effect, which may affect the uniformity or homogeneity. Secondly, symptomatic subjects were not included. Including symptomatic subjects reflects patients with LBP treated in physical therapy. Future studies of changes in mobility after applying manual force should include subjects with current complaints of low back pain to verify the results of this study. Third, this study only concentrated on the immediate effects of manual force. Lastly, possible measurement error should be considered, although our data were comparable to those of previous studies.
Conclusion
The result of current study demonstrated increased segmental and total ROM following the technique focusing on the segments with manual force. Despite this study still has limitations, positive effects of the technique with manual force on ROM were observed. Future research in this area is warranted.
References
- Pickar JG (2002) Neurophysiological effects of spinal manipulation. Spine J 2: 357-371.
- Maigne R (2006) Diagnosis and treatment of pain of vertebral origin. (2nd edn.), Taylor and Francis CRC press.
- Issacs ER, Bookhout MR (2002) Spinal Manipulation. (6thedn.), Butterworth/Heinemann.
- Pikula JR (1999) The effect of spinal manipulative therapy (SMT) on pain reduction and range of motion in patients with acute unilateral neck pain: a pilot study. J CanChiroprAssoc 43: 111-119.
- Whittingham W, Nilsson N (2001) Active range of motion in the cervical spine increases after spinal manipulation (toggle recoil). J Manipulative PhysiolTher 24: 552-555.
- Chiradejnant A, Latimer J, Maher CG, Stepkovitch N (2002) Dose the choice of spinal level treated during posteroanterior (PA) mobilisation affect treatment outcome. Physiotherapy Theory Pract 18: 165-174.
- Chiradejnant A, Maher CG, Latimer J, Stepkovitch N (2003) Efficacy of "therapist-selected" versus "randomly selected" mobilisation techniques for the treatment of low back pain: a randomised controlled trial. Aust J Physiother 49: 233-241.
- Ferna´ndez-de-las-Pen˜as C, Downey C, Miangolarra-Page JC (2005) Immediate changes in radiologically determined lateral flexion range of motion following a single cervical HVLA manipulation in patients with mechanical neck pain: A case series. Int J Osteopath Med 8: 139-145.
- Ferna´ndez-de-las-Pen˜as C, Palomeque-del-Cerro L, Rodrı´guez-Blanco C, Gómez-Conesa A, Miangolarra-Page JC (2007) Changes in neck pain and active range of motion after a single thoracic spine manipulation in subjects presenting with mechanical neck pain: A case series. J Manipulative PhysiolTher 30: 312-319.
- Martínez-Segura R, Fernández-de-las-Peñas C, Ruiz-Sáez M, López-Jiménez C, Rodríguez-Blanco C (2006) Immediate effects on neck pain and active range of motion after a single cervical high-velocity low-amplitude manipulation in subjects presenting with mechanical neck pain: a randomized controlled trial. J Manipulative PhysiolTher 29: 511-517.
- MacDonald CW, Whitman JM, Cleland JA, Smith M, Hoeksma HL (2006) Clinical outcomes following manual physical therapy and exercise for hip osteoarthritis: A case series. J Orthop Sports PhysTher 36: 588-599.
- Konstantinou K1, Foster N, Rushton A, Baxter D, Wright C, et al. (2007) Flexion mobilizations with movement techniques: the immediate effects on range of movement and pain in subjects with low back pain. J Manipulative PhysiolTher 30: 178-185.
- Powers CM, Beneck GJ, Kulig K, Landel RF, Fredericson M (2008) Effects of a single session of posterior-to-anterior spinal mobilization and press-up exercise on pain response and lumbar spine extension in people with nonspecific low back pain. PhysTher 88: 485-493.
- Yu H, Hou S, Wu W, He X (2011) Upper cervical manipulation combined with mobilization for the treatment of atlantoaxial osteoarthritis: a report of 10 cases. J Manipulative PhysiolTher 34: 131-137.
- Strunk RG, Hanses M (2011) Chiropractic care of a 70-year-old female patient with hip osteoarthritis. J Chiropr Med 10: 54-59.
- Powers CM, Kulig K, Harrison J, Bergman G (2003) Segmental mobility of the lumbar spine during a posterior to anterior mobilization: assessment using dynamic MRI. ClinBiomech (Bristol, Avon) 18: 80-83.
- Lee RY, McGregor AH, Bull AM, Wragg P (2005) Dynamic response of the cervical spine to posteroanteriormobilisation. ClinBiomech (Bristol, Avon) 20: 228-231.
- Kulig K, Landel RF, Powers CM (2004) Assessment of lumbar spine kinematics using dynamic MRI: A proposed mechanism of sagittal plane motion induced by manual posterior-anterior mobilization. J Orthop Sports Phys 34: 57-64.
- Krauss J, Creighton D, Ely JD, Podlewska-Ely J (2008) The immediate effects of upper thoracic translatoric spinal manipulation on cervical pain and range of motion: a randomized clinical trial. J Man ManipTher 16: 93-99.
- Kanlayanaphotporn R, Chiradejnant A, Vachalathiti R (2009) The immediate effects of mobilization technique on pain and range of motion in patients presenting with unilateral neck pain: a randomized controlled trial. Arch Phys Med Rehabil 90: 187-192.
- McGregor AH, Wragg P, Gedroyc WM (2001) Can interventional MRI provide an insight into the mechanics of a posterior-anterior mobilisation? ClinBiomech (Bristol, Avon) 16: 926-929.
- Intolo P, Milosavljevic S, Baxter DG, Carman AB, Pal P, et al. (2009) The effect of age on lumbar range of motion: a systematic review. Man Ther 14: 596-604.
- Thomas E, Silman AJ, Papageorgiou AC, Macfarlane GJ, Croft PR (1998) Association between measures of spinal mobility and low back pain. An analysis of new attenders in primary care. Spine (Phila Pa 1976) 23: 343-347.
- Mayer TG1, Robinson R, Pegues P, Kohles S, Gatchel RJ (2000) Lumbar segmental rigidity: can its identification with facet injections and stretching exercises be useful? Arch Phys Med Rehabil 81: 1143-1150.
- Mayer TG, Gatchel RJ, Keeley J, McGeary D, Dersh J, et al. (2004) A randomized clinical trial of treatment for lumbar segmental rigidity. Spine 29: 2199-2205.
- Al-Eisa E, Egan D, Deluzio K, Wassersug R (2006) Effects of pelvic skeletal asymmetry on trunk movement: three-dimensional analysis in healthy individuals versus patients with mechanical low back pain. Spine (Phila Pa 1976) 31: E71-79.
- Forbin W, Leivseth G, Biggemann M, Brinckmann P (2002) Sagittal plane segmental motion of the cervical spine. A new precision measurement protocol and normal motion data of healthy adults. ClinBiomech 17: 21-31.
- Wu SK, Kuo LC, Lan HC, Tsai SW, Chen CL, et al. (2007) The quantitative measurements of the intervertebral angulation and translation during cervical flexion and extension. Eur Spine J 16: 1435-1444.
- Sato T, Koumori T (2012) Preliminary Study of the Immediate Effect of Spinal Segmental Side Bending Mobilization on Improve Lumbar Range of Motion. J PhysTherSci 24: 431-434.
- Cardin AJ, Hadida C (1994) Evaluation of lumbar intersegmental range of motion using flexion-extension radiographs of asymptomatic versus low back pain adults. J CCA 38: 83-89.
- Dreischarf M1, Albiol L1, Rohlmann A1, Pries E1, Bashkuev M1, et al. (2014) Age-related loss of lumbar spinal lordosis and mobility - a study of 323 asymptomatic volunteers. PLoS One 9: e116186.
- Tarasevicius S, Kesteris U, Gelmanas A, Smailys A, Wingstrand H (2007) Intracapsular pressure and elasticity of the hip joint capsule in osteoarthritis. J Arthroplasty 22: 596-600.
- Tarasevicius S, Gelmanas A, Smailys A, Robertsson O, Wingstrand H (2009) Short rotator tendons do not increase intracapsular pressure in severe osteoarthritic hips. BMC MusculoskeletDisord 10: 12.
- Tarasevicius S, Kesteris U, Gelmanas A, Smailys A, Wingstrand H (2007) Intracapsular pressure and elasticity of the hip joint capsule in osteoarthritis. J Arthroplasty 22: 596-660.
- (2004) Paris SV: S1 Introduction to Spinal Evaluation and Manipulation. University of St. Augustine.
- Kalichman L, Hunter DJ (2007) Lumbar facet joint osteoarthritis: a review. Semin Arthritis Rheum 37: 69-80.
- Cohen SP, Stojanovic MP, Crooks M, Kim P, Schmidt RK, et al. (2008) Lumbar zygapophysial (facet) joint radiofrequency denervation success as a function of pain relief during diagnostic medical branch blocks: a multicenter analysis. Spine J 8: 498-504.
- Ribeiro LH, Furtado RN, Konai MS, Andreo AB, Rosenfeld A, et al. (2013) Effect of facet joint injection versus systemic steroids in low back pain: a randomized controlled trial. Spine 38: 1995-2002.
- Falco FJ, Manchikanti L, Datta S, Sehgal N, Geffert S, et al. (2012) An update of the systematic assessment of the diagnostic accuracy of lumbar facet joint nerve blocks. Pain Physician 15: E869-907.
- Bykowski JL, Wong WH (2012) Role of facet joints in spine pain and image-guided treatment: a review. AJNR Am J Neuroradiol 33: 1419-1426.
- Mayer TG, Tencer AF, Kristoferson S, Mooney V (1984) Use of noninvasive techniques for quantification of spinal range-of-motion in normal subjects and chronic low-back dysfunction patients. Spine (Phila Pa 1976) 9: 588-595.
- Mayer T, Tabor J, Bovasso E, Gatchel RJ (1994) Physical progress and residual impairment quantification after functional restoration. Part I: Lumbar mobility. Spine (Phila Pa 1976) 19: 389-394.
- TANZ SS (1953) Motion of the lumbar spine; a roentgenologic study. Am J Roentgenol Radium TherNucl Med 69: 399-412.
- Pearcy MJ, Tibrewal SB (1984) Axial rotation and lateral bending in the normal lumbar spine measured by three-dimensional radiography. Spine 9: 582-587.
- Panjabi MM, Oxland TR, Yamamoto I, Crisco JJ (1994) Mechanical behavior of the human lumbar and lumbosacral spine as shown by three-dimensional load-displacement curves. J Bone Joint Surg Am 76: 413-424.
- Steffen T, Rubin RK, Baramki HG, Antoniou J, Marchesi D, et al. (1997) A new technique for measuring lumbar segmental motion in vivo. Method, accuracy, and preliminary results. Spine (Phila Pa 1976) 22: 156-166.
Relevant Topics
- Child Health Education
- Construction Safety
- Dental Health Education
- Holistic Health Education
- Industrial Hygiene
- Nursing Health Education
- Occupational and Environmental Medicine
- Occupational Dermatitis
- Occupational Disorders
- Occupational Exposures
- Occupational Medicine
- Occupational Physical Therapy
- Occupational Rehabilitation
- Occupational Standards
- Occupational Therapist Practice
- Occupational Therapy
- Occupational Therapy Devices & Market Analysis
- Occupational Toxicology
- Oral Health Education
- Paediatric Occupational Therapy
- Perinatal Mental Health
- Pleural Mesothelioma
- Recreation Therapy
- Sensory Integration Therapy
- Workplace Safety & Stress
- Workplace Safety Culture
Recommended Journals
Article Tools
Article Usage
- Total views: 17745
- [From(publication date):
April-2015 - Dec 12, 2024] - Breakdown by view type
- HTML page views : 13250
- PDF downloads : 4495