Research Article Open Access
Demographic patterns of Acoustic Shock syndrome as seen in a large call centre
Ayugi John, Loyal Poonamjeet*, Mugwe Peter and Nyandusi MusaDepartment of Human Anatomy, University of Nairobi, Nairobi, Kenya
- *Corresponding Author:
- Poonamjeet Loyal
Department of Human Anatomy
University of Nairobi, Nairobi
Kenya
Tel: 752381860
E-mail: kaurpoonamjeet@ gmail.com
Received date: July 20, 2015; Accepted date: August 13, 2015; Published date: August 21, 2015
Citation: John A, Poonamjeet L, Peter M, Musa N (2015) Demographic Patterns of Acoustic Shock Syndrome as Seen in a Large Call Centre. Occup Med Health Aff 3:212. doi: 10.4172/2329-6879.1000212
Copyright: © 2015 John A, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Visit for more related articles at Occupational Medicine & Health Affairs
Abstract
Call centers represent one of the fastest growing industries in East Africa. However, there are health and safety hazards unique to this new industry. This field is underexplored for workers of call centers in East Africa and this study sought to establish the presence of acoustic shock syndrome, the age and sex characteristics of the staff involved and to determine correlation between duration of exposure and development of Acoustic shock syndrome. In a descriptive cross-sectional study, a total of 1351 employees, male 579 and female 772 subjects were recruited. They were screened for Acoustic shock syndrome. The age group of the subjects for this study ranged from 19-55 years. Those subjects with other medical conditions were excluded. The subjects were screened for acoustic shock syndrome using a questionnaire and the age, sex and duration of work was also sort. The total number of people with Acoustics shock syndrome were 385. This study has noted that 13% of workers at call centers develop Acoustic Shock syndrome irrespective of their duration of exposure. Males and females are affected equally. The peak groups affected are those with 3 and 5 years of work experience. Methods of noise measurement in such work environments need to be implemented so that a time weighted average can be established for protection of exposed workers.
Keywords
Call centers; Acoustic shock syndrome; Demographic; Depression
Introduction
Acoustic shock is an involuntary response to a sound perceived as traumatic (acoustic incident), which causes a specific and consistent pattern of neurophysiological and psychological symptoms. These include aural pain, tinnitus, hyperacusis/phonophobia, vertigo and other unusual symptoms such as numbness or burning sensations around the ear. A range of emotional reactions including trauma, anxiety and depression can develop [1].
The symptoms of Acoustic shock are usually temporary, but some may persist with ensuing permanent disability. The term acoustic shock disorder (ASD) is used to identify this persistent symptom cluster
An acoustic incident is any sound that is perceived as threatening, usually a sudden/unexpected/loud sound heard near the ear. The sound is rarely loud enough or present for long enough to cause a noise induced hearing loss.
A call center is defined as a workstation where the basic tasks of a worker are carried out with the use of a phone and a computer. According to statistics, about 1.3-4% of workers are employed in call centers in the European countries. The number employed in Subsaharan Africa is rising yet occupational health measures to protect workers from harmful noise remains wanting [2]. Call centre staff using a telephone headset are vulnerable to ASD because of the increased likelihood of exposure, close to their ear(s), to an acoustic incident randomly transmitted via the telephone line. The objective of this paper is to study the magnitude of the Acoustic shock syndrome in a big call center in East Africa.
Materials and Methods
In a descriptive cross -sectional study, a total of 1351 employees, male 579 and female 772 subjects were recruited. They were screened for Acoustic shock syndrome. The age group of the subjects for this study ranged from 19-55 years. Those subjects with other medical conditions were excluded. The subjects were screened for acoustic shock syndrome and duration of work and demographic details were put in.
Results
The total number of people recruited for this study was 1351 employees, male 579 and female 772 subjects and 385 had acoustic shock syndrome. The results showed a bimodal distribution regarding the people who developed Acoustic Shock syndrome and their number of years at work 2 peaks: those who had worked for 3 years and those that had worked for 5 years (Figure 1). The number of people with acoustic shock syndrome declined as the number of years worked exceeded 5 years. Nine or more years at work saw the least number of people with acoustic shock syndrome. Furthermore, gender bias towards the female gender was seen with 53% females and 47% of males developing acoustic shock syndrome. These were however not statistically significant at 95% confidence interval p value of 0.05 (Table 1).
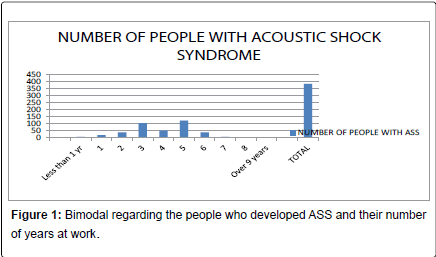
Figure 1: Bimodal regarding the people who developed ASS and their number of years at work.
| Years worked | Number of people with ASS | Percentage of people with ASS |
| Less than 1 yr | 6 | 1.56 |
| 1 | 18 | 4.68 |
| 2 | 37 | 9.61 |
| 3 | 104 | 27.01 |
| 4 | 50 | 12.99 |
| 5 | 121 | 31.43 |
| 6 | 37 | 9.61 |
| 7 | 6 | 1.56 |
| 8 | 4 | 1.04 |
| Over 9 years | 2 | 0.52 |
| Total | 385 | 100 |
Table 1: Percentage of people with acoustic shock syndrome and the number of
years worked.
Discussion
Call Centre telephone operators experience acoustic incidents such as a sudden loud shriek or piercing tone through their headsets [3]. ACIFG616: 2004, Guideline-Acoustic Safety for Telephone Equipment, defines an acoustic incident as: The receipt by a telephone user of an unexpected sound that has acoustic characteristics that may cause an adverse reaction in some telephone users [4]. Depending on the characteristics of the sound and the user, an acoustic shock may result from the incident which is defined by ACIFG616: 2004 as: Any temporary or permanent disturbance of the functioning of the ear, or of the nervous system, which may be caused to the user of a telephone earphone by a sudden sharp rise in the acoustic pressure produced by it [5].
The initial physiological symptoms of acoustic shock are considered to be a direct consequence of excessive, involuntary middle ear muscle contractions. While the stapedial reflex is an acoustic reflex triggered by high volume levels, the tensor tympani reflex is a startle reflex [6] which is exaggerated by high stress levels. The tensor tympani muscle contracts immediately preceding the sounds produced during selfvocalization, suggesting it has an established protective function to loud sounds [7], assists in the discrimination of low frequency sounds, and is involved in velopharyngeal movements [8].
This study found that 384 (13%) workers at the Call center developed Acoustic shock syndrome irrespective of their duration at work. The results had a bimodal distribution with the maximum number of people developing acoustic shock syndrome after 3 and 5 years of work. We postulate that it takes 3 years for Acoustic shock syndrome to develop and the workers may be taking a work leave to recuperate. This could explain the drop in the number of cases after work duration of 4 years. The second peak at 5 years could be a result of recurrence of Acoustic Shock Syndrome after the workers report back to work after their leave. Further studies are however needed to prove this hypothesis
Conclusion
The total number of people with Acoustics shock syndrome were 385. This study has noted that 13% of workers at call centers develop Acoustic Shock syndrome irrespective of their duration of exposure [9]. Males and females are affected equally. The peak groups affected are those with 3 and 5 years of work experience. Methods of noise measurement in such work environments need to be implemented so that a time weighted average can be established for protection of exposed workers.
References
- Westcott M (2006) Acoustic Shock Injury. ActaOtol Supplement556: 54-58
- BozenaSmagowska (2010)Noise at Workplaces in the Call Center. Archives of Acoustics 35:253-264
- Chiusano SV, Lees PSJ, Breysse PN (1995) An occupational noise exposure assessment for headset-wearing communications workers Appl Occup Environ Hyg 10:476-481.
- Patel JA, Broughton K (2002) Assessment of the noise exposure of call centre operators. AmOccupHyg 46: 653-661
- Peretti A, Pedrielli F, Baiamonte M, Mauli F, Farina A (2003) Headphone noise: occupational noise exposure assessment for communication personnel, Euronoise, Naples 2003, paper ID: 365-IP/p1
- Milhinch JC (2001) Acoustic Shock Injury - A report on injury following acoustic incidents in call centres. Melbourne (personal communication)
- Ramirez LM, Ballesteros LE, Sandoval GP (2007) Tensor tympani muscle: strange chewing muscle Med Oral Patol Oral Cir Bucal 12: E96-100
- Patuzzi R (2002) Acute Aural Trauma in Users of Telephone Headsets and Handsets. In: Ching T editor. Abstracts of XXVI International Congress of Audiology, Melbourne 17th-21st March 2002. Aust N Z J Audiol (spec ed) 23(2):132.
- Groothoff B (2005) Acoustic shock in call centres. Proceedings of ACOUSTICS 2005 9-11, Busselton, Western Australia Australian Acoustical Society 335. Workplace Health and Safety Queensland, Level 4/ 543 Lutwyche Road, LutwycheQld 4030, Australia
Relevant Topics
- Child Health Education
- Construction Safety
- Dental Health Education
- Holistic Health Education
- Industrial Hygiene
- Nursing Health Education
- Occupational and Environmental Medicine
- Occupational Dermatitis
- Occupational Disorders
- Occupational Exposures
- Occupational Medicine
- Occupational Physical Therapy
- Occupational Rehabilitation
- Occupational Standards
- Occupational Therapist Practice
- Occupational Therapy
- Occupational Therapy Devices & Market Analysis
- Occupational Toxicology
- Oral Health Education
- Paediatric Occupational Therapy
- Perinatal Mental Health
- Pleural Mesothelioma
- Recreation Therapy
- Sensory Integration Therapy
- Workplace Safety & Stress
- Workplace Safety Culture
Recommended Journals
Article Tools
Article Usage
- Total views: 17791
- [From(publication date):
August-2015 - Jul 11, 2025] - Breakdown by view type
- HTML page views : 13023
- PDF downloads : 4768