Adhesive Capsulitis and Tendinopathy: Evolution of Sinergy of MyofascialRelease Conjugated With Photobiomodulation after 60 Days
Received: 01-Feb-2024 / Manuscript No. jnp-24-127935 / Editor assigned: 03-Feb-2024 / PreQC No. jnp-24-127935(PQ) / Reviewed: 17-Feb-2024 / QC No. jnp-24-127935 / Revised: 22-Feb-2024 / Manuscript No. jnp-24-127935(R) / Published Date: 29-Feb-2024 DOI: 10.4172/2165-7025.1000674
Abstract
The shoulder is a very complex joint, and it is necessary that all structural structures are synchronized, because if they present alterations, the joint complex will be the target of numerous conditions, including tendinopathy and adhesive capsulitis. Tendinopathy is characterized by mechanical impaction or compression of certain structures, which may present inflammation, degeneration in the tendons; adhesive capsulitis occurs in changes in the joint capsule, providing chronic inflammation and adhesion, generating pain and limitation in the range of motion of the joint. Through this, researchers from the Physics Institute of São Carlos, University of São Paulo, developed new equipment that combines technologies, allowing the synergy of myofascial release and photobiomodulation therapies, obtaining positive results in terms of improving pain, inflammation and range of movement. The objective of this study was to monitor and compare the after treatment evolution and the effect after the 60-day period in patients with tendinopathy and adhesive capsulitis, using respectively the goniometric measurement of joint angles, the visual analogy scale and the Questionnaire of Dysfunctions of the Arm, Shoulder and Hand. The singular myofascial release and photobiomodulation treatments and the synergic use of these same resources were compared and analysed, pre-treatment, after treatment and after 60 days. As a result, the synergic treatment with myofascial release and photobiomodulation proved to be effective even after 60 days of intervention, confirming the new physical therapy approach as the best treatment option for these shoulder injuries, allowing the return of quality of life without the use of drugs or invasive techniques.
Keywords
Adhesive capsulitis; Tendinopathy; Myofascial release; Photobiomodulation
Introduction
The shoulder is a very complex joint, which may present some instability, which makes it more susceptible to the presence of numerous conditions, including tendinopathy and adhesive capsulitis [1].
Tendinopathy is a condition attributed to mechanical factors where repetitive efforts, trauma and excessive use of the joint are predominant, generating inflammation and injuries in soft structures, and also to a vascular factor where there is a deficient blood supply in the tendons, suffering degenerative changes [2]. The estimated prevalence is 29%, affecting mainly women, between 40 and 50 years of age and continues to grow after 70 years of age [3].
In the case of adhesive capsulitis, which is a condition of unknown cause, it can be associated with a traumatic, mechanical episode or by repetitive strain, providing a chronic inflammation of the joint capsule, with fibrosis and adhesion generating pain and limitation in the range of motion of the joint due to long periods of immobility, reaching a general population of 3 to 5%, affecting more females (2:1) in the age group from 40 to 60 years [4-6].
Shoulder problems affect functional recovery and functional use of the arm, which decreases performance and autonomy in daily life, such as putting on a jacket or coat, putting objects in back pockets, in the case of women, closing the bra behind the back, practice in personal care (such as brushing teeth, washing the face, combing the hair), taking cutlery to the mouth, lifting heavy objects and limitation to perform repetitive activities [7].
Regarding the treatments of these conditions, there are several, such as pharmacological, physiotherapeutic and also alternative treatments,such as acupuncture, massages, among others. In the case of physical therapy, the objective of this treatment is to improve pain control, the inflammatory response, relaxing the muscles, thus providing a functional improvement to the individual [8].
In recent years, researchers from the Physics Institute of São Carlos, University of São Paulo (IFSC-USP) have been developing projects and publishing articles with positive results, on combined technologies, associating two physiotherapeutic resources for simultaneous use, making it possible to overlap the area of action of the two resources [9-12].
Through these new technologies combined, a new equipment already approved by ANVISA (Brazilian National Health Surveillance Agency), the RollerLaser, with internationally published articles on conditions such as adhesive capsulitis and tendinopathy [13,14] and repetitive strain injuries in the upper limbs [15], which performs synergistically a mechanical action and light action, where the mechanical action consists of a myofascial release technique, through muscle compression, deep sliding and friction movement used, reorganizing, restoring and aligning the function between the fascia and the muscle, providing a dilation of blood vessels, favouring greater vitality and flexibility of skin tissues, eliminating muscle tension, providing a calming effect, thus improving range of motion and pain in the affected limb [16].
And the action of light, which corresponds to photobiomodulation, stimulating the cytochrome-c-oxidase photoreceptor, resulting in increased metabolism and energy production, consequently increasing mitochondrial oxidative metabolism and initiating a cascade of cellular reactions that modulate biological behaviour, angiogenesis, macrophages and lymphocytes, providing an analgesic and inflammatory response, as well as the proliferation of fibroblasts, collagen synthesis and the differentiation of mesenchymal cells into osteoblasts, among others, thus accelerating the tissue regeneration process [17].
Therefore, the aim of this study was to monitor and compare the post-treatment evolution and the effect after the 60-day period in patients with tendinopathy and adhesive capsulitis.
Materials and Methods
Approval of the research ethics committee
This study has two approvals from human research ethics committees, under C.A.A.E. number 40296320.5.0000.8148 for adhesive capsulitis and C.A.A.E number 55137522.4.0000.8148 for tendinopathy, both following resolutions 466/2012 and 510/2016. The study was carried out at the Photodynamic Therapy Unit at Hospital Santa Casa, in São Carlos, a clinical research unit in partnership with the São Carlos Institute of Physics at the University of São Paulo. All procedures were obtained through free and informed consent.
Equipment
The equipment was developed by the Technical Support Laboratory (TSL) of the Institute of Physics of São Carlos (IFSC), and approved by Brazilian Health Regulatory Agency (ANVISA) and is already being marketed by the company MMOptics from São Carlos. The equipment has in its geometry, two spheres at the ends, which with the mechanical action compress the muscle with the help of the spheres, together with the circular movements performed by them, rubbing the skin, and a deep slide, covering the entire extension of the muscle, together with the action of light, the wavelength and time that will be applied are adjusted on the device's display (Figure 1, Figure 2).

Figure 1: Illustration of the RollerLaser equipment, myofascial laser equipment, composed of two lateral spheres and centrally, the laser emission in the 660nm and 808nm wavelengths.

Figure 2: Illustrations of the equipment, where it is possible to observe the synergy of the mechanical action and the action of light on the affected shoulder muscles, always performing the movement in the direction of the muscle fibers.
Clinical research and protocol
The study population consisted of 30 patients, 15 patients with tendinopathy and 15 patients with Adhesive Capsulitis, divided into 6 groups (n=5), shown in Figure 3. Were select patients of both sexes, aged between 30 and 70 years old.

Figure 3: Experimental design performed. There were 10 intervention sessions and follow-up 60 days after the intervention.
In the application of the laser, the wavelength of 808nm-infrared was used. All treatments were performed 2 times a week, for 15 minutes for a period of 10 sessions, covering the muscles of the compromised shoulder.
Evolution assessment mechanisms
The evaluation of the Visual Analogue Scale (VAS) pain scale was performed for the pre-treatment, after treatment (10 sessions) and after 60 days, whose scale varies from 0 to 10, where the patient indicates how much pain he is feeling.
The Arm, Shoulder and Hand Dysfunction Questionnaire (DASH), which aims to measure the symptoms and abilities of individuals with musculoskeletal pathologies in the upper limbs. Calculating the DASH score: To calculate the score for the 30 questions, the following formula must be used: (Sum of the values for the 30 questions – 30/1.2. A high score indicates major dysfunction.
Statistic
Data were submitted to a Kolmogorov Smirnov normality test and later to an Anova Two Away analysis, using Tukey Kramer's post-Hoc test to analyse the evolution, considering p<0.05. The software used was Instat 3.0 for Windows.
Results
The results obtained were compared before and after treatment with Roller, Laser and RollerLaser, in patients affected by Adhesive Capsulitis in relation to movements of flexion, extension, abduction, adduction, internal rotation and external rotation of the shoulder, EVA and DASH, with data percentages expressed as mean and standard error, using the Kolmogorov-Smirnov normality test and subsequently the Anova Two Away analysis, to compare evolution (Table 1). There was a significant difference in the pre and post comparison of Roller treatment, in flexion (p<0.009), abduction (p<0.01), external rotation (p<0.02), VAS (p<0.002) and DASH (p<0.007) movements. There was a difference in the percentage in the pre and post comparison of Roller treatment, in flexion movements (9.94%), extension (5.55%), abduction (16%), adduction (5.3%), internal rotation (24.5%), external rotation (25.4%), EVA (-69%) and DASH (-29.5%).
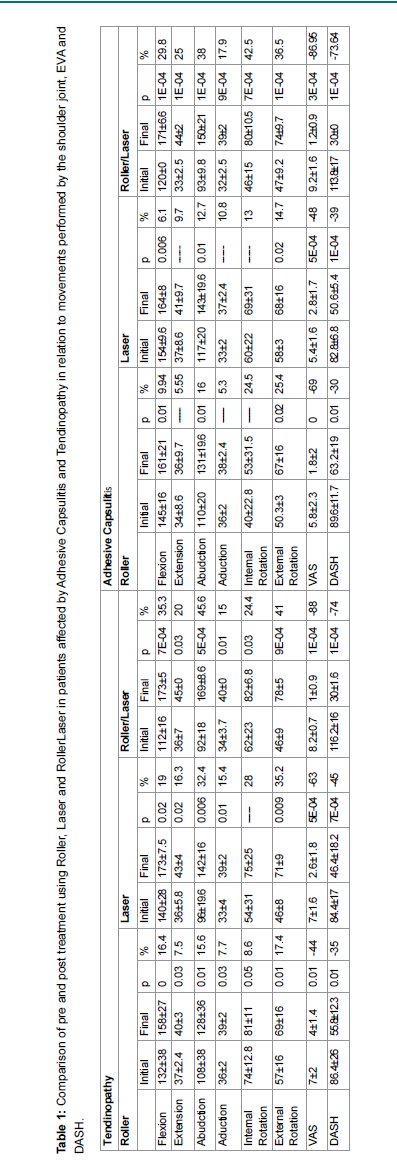
There was a significant difference in the before and after comparison of the Laser treatment, in the movements of flexion (p<0.006), abduction (p<0.01), external rotation (p<0.02), VAS (p<0.0005) and DASH (p<0.0001). There was a difference in the percentage in the comparison before and after the Laser treatment, in flexion movements (6.1%), extension (9.7%), abduction (12.7%), adduction (10.8%), internal rotation (13%), external rotation (14.7%), EVA (- 48.1%) and DASH (- 39%).
There was a significant difference in the before and after comparison of RollerLaser treatment, in the movements of flexion (p<0.0001), extension (p<0.0001), abduction (p<0.0001), adduction (p<0.0009), internal rotation (p<0.0007), external rotation (p<0.0001), EVA (p<0.0003) and DASH (p<0.0001). There was a difference in percentage in the pre and post comparison of RollerLaser treatment, in flexion movements (29.8%), extension (25%), abduction (38%), adduction (17.9%), internal rotation (42.5%), external rotation (36.5%), EVA (- 86.95%) and DASH (- 73.64%).
Regarding the results obtained, when comparing the before and after treatment values of Roller, Laser and RollerLaser, in patients affected by Tendinopathy according to the movements of flexion, extension, abduction, adduction, internal rotation and external rotation of the shoulder, VAS and DASH, with percentage data expressed as mean and standard error, using the Kolmogorov-Smirnov normality test and subsequently the Anova Two Away analysis, to compare evolution. There was a significant difference in the pre and post comparison of the Roller treatment, in the movements of flexion (p<0.001), extension (p<0.03), abduction (p<0.01), adduction (p<0.03), internal rotation (p<0.05), external rotation (p<0.01), EVA (p<0.007) and DASH (p<0.005). There was a difference in percentage in the before and after comparison of Roller treatment, in flexion (16.4%), extension (7.5%), abduction (15.6%), adduction (7.7%), internal rotation (8.6%), external rotation movements (17.4%), EVA (- 44.4%) and DASH (- 35.4%).
A significant difference was observed in the before and after comparison of the Laser treatment, in the movements of flexion (p<0.02), extension (p<0.02), abduction (p<0.006), adduction (0.01), external rotation (p<0.009), VAS (p<0.0005) and DASH (p<0.0007). There was a difference in the percentage in the comparison before and after the Laser treatment, in flexion movements (19%), extension (16.3%), abduction (32.4%), adduction (15.4%), internal rotation (28%), external rotation (35.2%), EVA (- 62.8%) and DASH (- 45.0%).
There was a significant difference in the before and after comparison of RollerLaser treatment, in the movements of flexion (p<0.0007), extension (p<0.03), abduction (p<0.0005), adduction (p<0.01), internal rotation (p<0.03), external rotation (p<0.0009), EVA (p<0.0001) and DASH (p<0.0001). There was a difference in the percentage in the pre and post comparison of RollerLaser treatment, in flexion movements (35.3%), extension (20%), abduction (45.6%), adduction (15%), internal rotation (24.4%), external rotation (41%), EVA (- 87.8%) and DASH (- 73.5%) (Table 1).
The results obtained were compared to the treatment performed with Roller in the before treatment, after treatment and after 60 days, for adhesive capsulitis and tendinopathy. Kolmogorov-Smirnov normality test and subsequent Tukey-Kramer post-hoc test for p<0.05 were performed, in the comparisons it was shown that before treatment x after treatment and before treatment x after 60 days there was a statistically significant difference for both adhesive capsulitis and for tendinopathy (#before Treatment x after Treatment in Adhesive Capsulitis (p<0.01) and in the comparison ##Before Treatment x After 60 days in Adhesive Capsulitis (p<0.01), #Before Treatment x After Treatment in Tendinopathy (p<0.02) and in the comparison ##Before Treatment x After 60 days in Tendinopathy (p<0.02), the percentage difference was also expressed *Before Treatment x After Treatment and **Before Treatment x After 60 This analysis also emphasized the difference in the percentage of the groups analysed, *Before Treatment x After Treatment in Adhesive Capsulitis (68.9%) and in the percentage **Before Treatment x After 60 days in Adhesive Capsulitis (65.5%). There was a difference in the percentage *Before Treatment x After Treatment in Tendinopathy (44.4%) and in the percentage **Before Treatment x After 60 days in tendinopathy (33.3%) (Figure 4).

Figure 4: Comparison of the treatment performed with Roller in the before treatment, after treatment and after 60 days, for adhesive capsulitis and tendinopathy. Kolmogorov-Smirnov normality test and subsequent Tukey-Kramer post-hoc test was performed for p<0.05, in the comparisons #Before Treatment x After Treatment, ##Before Treatment x After 60 days and ### After Treatment x After 60 days. Also, a percentage difference was expressed *Before Treatment x After Treatment and **After Treatment x After 60 days.
Comparing the treatment performed with Laser in the before treatment, after treatment and after 60 days, for adhesive capsulitis and tendinopathy. Kolmogorov-Smirnov normality test and subsequent Tukey-Kramer post-hoc test for p<0.05 were performed, in the comparisons it was shown that before treatment x after treatment and before treatment x after 60 days there was a statistically significant difference for both adhesive capsulitis and tendinopathy (#Before Treatment x After Treatment in Adhesive Capsulitis (p<0.003), ##Before Treatment x After 60 days in Adhesive Capsulitis (p<0.003).
#Before Treatment x After Treatment in Tendinopathy (p<0.003) and ##Before Treatment x After 60 days in tendinopathy (p<0.003). Also, the percentage difference *Before Treatment x After Treatment and **Before Treatment x after 60 days was expressed. There was a difference in the percentage *Before Treatment x After Treatment in Adhesive Capsulitis (48.1%) and in the percentage **Before Treatment x After 60 days in Adhesive Capsulitis (37%). There was a difference in the percentage *Before Treatment x After Treatment in Tendinopathy (62.8%) and in the percentage **Before Treatment x After 60 days in Tendinopathy (51.4%) (Figure 5).

Figure 5: Comparison of the treatment performed with Laser in the before treatment, after treatment and after 60 days, for adhesive capsulitis and tendinopathy. Kolmogorov-Smirnov normality test and subsequent Tukey-Kramer post-hoc test was performed for p<0.05, in the comparisons # before Treatment x after Treatment, ##Before Treatment x After 60 days and ### After Treatment x After 60 days. Also, a percentage difference was expressed *Before Treatment x After Treatment and ** Before Treatment x After 60 days.
Comparing the treatment performed with RollerLaser in the before treatment, after treatment and after 60 days, for adhesive capsulitis and tendinopathy. Kolmogorov-Smirnov normality test and subsequent Tukey-Kramer post-hoc test for p<0.05 were performed, in the comparisons it was shown that before treatment x after treatment and before treatment x after 60 days there was a statistically significant difference for both adhesive capsulitis and for tendinopathy (#Before Treatment x After Treatment in Adhesive Capsulitis (p<0.001),##Before Treatment x After 60 days in Adhesive Capsulitis (p<0.001), #Before Treatment x After Treatment in Tendinopathy (p<0.0001) and ##Before Treatment x After 60 days in tendinopathy (p<0.0001).
Also, the percentage difference *Before Treatment x After Treatment and **Before Treatment x after 60 days was expressed. There was a difference in the percentage *Before Treatment x After Treatment in Adhesive Capsulitis (86.9%) and in the percentage **Before Treatment x After 60 days in Adhesive Capsulitis (89.1%). There was a difference in the percentage *Before Treatment x After Treatment in Tendinopathy (87.8%) and in the percentage **Before Treatment x After 60 days in Tendinopathy (85.4%) (Figure 6).

Figure 6: Comparison of the treatment performed with RollerLaser in the before treatment, after treatment and after 60 days, for adhesive capsulitis and tendinopathy. Kolmogorov-Smirnov normality test and subsequent Tukey-Kramer post-hoc test was performed for p<0.05, in the comparisons #Before Treatment x After Treatment, ##Before Treatment x After 60 days and ### After Treatment x After 60 days. Also, a percentage difference was expressed *Before Treatment x After Treatment and **Before Treatment x After 60 days.
Discussion
Tendinopathy is characterized by mechanical factors through excessive use of the upper limb and also by vascular factors, causing pain, inflammation and degeneration in the tendon, and partial and total ruptures in the tendons may occur, providing restriction of the movements of the shoulder joint complex, which they may also be accompanied by other alterations, such as tendinous calcifications, glenohumeral and acromioclavicular osteoarthritis, and adhesive capsulitis [18]. Adhesive capsulitis is distinguished by a chronic inflammation of the joint capsule, with fibrosis and adhesion, generating pain and limitation in the range of motion of the shoulder joint [4].
With this, the synergistic use of the mechanical action and the light action of the RollerLaser equipment, performs a myofascial release technique, which through the combination of three movements, compression, sliding, friction, provide the stretching of the muscles and the reorganization of the fascia, with the ultimate goal of tissue relaxation and analgesia [16]. While photobiomodulation interacting with biological tissue, an electronic excitation will follow, which in turn will stimulate cellular functions, such as the cytochrome-c-oxidase photoreceptor, resulting in increased ATP (Adenosine Triphosphate) production, providing the acceleration of microcirculation? Tissue and cell proliferation, promoting therapeutic effects such as analgesic, antiinflammatory and tissue regeneration effects [17].
Previous studies with great evolution on the synergistic use of laser treatments and myofascial release, is increasingly authentic for inflammatory and degenerative treatments. One of these studies uses the new technology in patients with adhesive capsulitis and tendinopathy, presenting relevant results, such as improvement in pain, inflammation and also in range of motion, in a reduced treatment time, thus demonstrating a great therapeutic action [13,14]. Another study that applied the synergistic action of photobiomodulation and the myofascial release technique in patients with repetitive strain injuries, in the studied pathologies such as neck pain, myofascial trigger points, supraspinatus tendinitis, lateral and medial epicondylitis and carpus, obtained positive responses in all pathologies, promoting and favouring the return to functionality and improved quality of life for the patient [14].
However, we ended the study by monitoring and comparing the treatments performed with Roller, Laser and RollerLaser in the pre-treatment, post-treatment and after 60 days in patients with tendinopathy and adhesive capsulitis, noting that the synergistic treatment using myofascial release and photobiomodulation presented great therapeutic relevance after a period of 60 days, allowing full restoration of movement and absence of pain.
In this way, the combined action of myofascial release and laser enables a new and effective form of treatment for shoulder injuries, allowing full restoration of movement and absence of pain.
Conclusion
The synergistic treatment using myofascial release and photobiomodulation showed great therapeutic relevance after a period of 60 days in patients with adhesive capsulitis and tendinopathy, showing that this new technology for these pathologies can obtain expressive results in a shorter time and maintain the result even considering a period after the intervention, providing the patient with an efficient non-pharmacological treatment, with action on pain, inflammation and limitation of movements, allowing the return of well-being and quality of life to the patient.
Acknowledgment
This work was supported by São Paulo Research Foundation (FAPESP – grants n◦2013/07276-1 and 2014/50857-8) and by National Council for Scientific and Technological Development (CNPq – grant n◦ 465360/2014-9).
References
- Linaker CH, Walker-Bone K (2015) Shoulder disorders and occupation. Best Pract Res Clin Rheumatol 29: 405-423.
- Rees JD, Wilson AM, Wolman RL (2006) Current concept sin the management of tendon disorders. Rheumatology 45: 508-521.
- Van Der Windt DA, Koes BW, de Jong BA, Bouter LM (1995) Shoulder disorders in general practice: incidence, patient characteristics,andmanagement. Ann Rheum Dis 54: 959-964.
- Redler L, Dennis E (2019) Treatment of Adhesive Capsulitis of Shoulder. J Am Acad Orthop Surg 27: 544-554.
- Neviaser AS, Neviaser RJ (2011) Adhesive Capsulitis of the Shoulder. J Am Acad Orthop Surg 19: 536-542.
- Ramirez J (2019) Adhesive Capsulitis: Diagnosis and Management. Am Fam Physician 99: 297-300.
- Lindgren I, Jonsson AC, Norrving B, Lindgren A (2007) Shoulder Pain after Stroke: A Prospective Population-Based Study. Stroke 38: 343–348.
- Page P, Labbe A (2010) Adhesive Capsulitis: Use the evidence to integrate your interventions. Nam J Sports Phys Ther 5: 266-73.
- De Souza Simao ML, Fernandes AC, Ferreira KR, De Oliveira LS, Mario EG, et al. (2019) Comparison between the Singular Action and the Synergistic Action of Therapeutic Resources in the Treatment of Knee Osteoarthritis in Women: A Blind and Randomized Study. J Nov Physiother 9: 1-3.
- Junior AEA, Carbinatto FM, Franco DM, Bruno JSA, Simao MLS, et al. (2020) The Laser and Ultrasound: The Ultra Laser like Efficient Treatment to Fibromyalgia by Palms of Hands–Comparative Study. J Nov Physiother 11: 1-5.
- Tamae PE, Dos Santos AV, Simão MLS, Canelada ACN, Zampieri KR, et al. (2020) Can the associated use of negative pressure and laser therapy be a new and efficient treatment for Parkinson’s pain? A comparative study. J Alzheimers Dis Parkinsonism 10: 1-6.
- Panhóca VH, Nogueira MS, Bagnato VS (2020) Treatment of facial nerve palsies wit laser and endermotherapy: a report of two cases. Laser Phys 18: 15601.
- Canelada ACN, Carbinatto FM, de Aquino Junior AE, Bagnato VS (2021) A Case Report on the Use of a Conjugated System ofMyofascialRelease for Shoulder Capsulitis. J Nov Physiother 11: 476.
- Canelada ACN, Vitor Hugo Panhóca, Carbinatto FM, Bagnato VS, De Aquino Junior AE (2022) Can a new synergistic proposal involving photobiomodulation and myofascial release accelerate the evolution of adhesive capsulitis and tendinopathies? J Nov Physiother 12: 535.
- Canelada ACN, De Aquino Junior AE, Carbinatto FM, Panhóca VH, Simão G, et al. (2022) The Synergy of Photobiomodulation and Myofascial Release in Upper Limb Injuries-Case Series. J Nov Physiother 12: 515.
- Ajimsha MS, Al-Mudahka Nr, Al-Madzhar JA (2015) Effectiveness of myofascial release: Systematic review of randomized controlled trails. J Bodyw Mov Ther 19: 102-112.
- Karu TL (2000) Mechanisms of low-power laser light action on cSellular level. In: Karu, T.I. & Lubart, R. Effects of low-power light on biological systems V. Amsterdam, Netherlands: Proceedingsof SPIE 4159: 01-17.
- Dong W, Goost H, Lin X, Burger C, Paul C, et al. (2015) Treatments for Shoulder Impingement Syndrome: Aprisma Systematic Reviewand Network Meta Analysis. Medicine 94:10.
Indexed at, Google Scholar, Crossref
Indexed at, Google Scholar, Crossref
Indexed at, Google Scholar, Crossref
Indexed at, Google Scholar, Crossref
Indexed at, Google Scholar, Crossref
Indexed at, Google Scholar, Crossref
Indexed at, Google Scholar, Crossref
Indexed at, Google Scholar, Crossref
Indexed at, Google Scholar, Crossref
Citation: Canelada ACN, Carbinatto FM, Bagnato VS, Junior AEA (2024) Adhesive Capsulitis and Tendinopathy: Evolution of Sinergy of Myofascial Release Conjugated With Photobiomodulation after 60 Days. J Nov Physiother 14: 674. DOI: 10.4172/2165-7025.1000674
Copyright: © 2024 Canelada ACN, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Select your language of interest to view the total content in your interested language
Share This Article
Recommended Journals
Open Access Journals
Article Tools
Article Usage
- Total views: 1980
- [From(publication date): 0-2024 - Nov 26, 2025]
- Breakdown by view type
- HTML page views: 1632
- PDF downloads: 348