A Case Whose Intermittent Claudication Disappeared After Weight Reduction
Received: 05-Jun-2018 / Accepted Date: 11-Jun-2018 / Published Date: 12-Jun-2018 DOI: 10.4172/2165-7025.1000394
Abstract
A 58-year-old male (162.1 cm, 76.8 kg, body mass index 29.2) suffered from intermittent claudication. At the initial visit, walking 10-100 meters caused pain in lateral part of the right lower limb, resulting in inability to walk. Xray showed mild forward slip of the fifth lumbar vertebra, however, MRI did not show narrowing of the lumbar canal. He could walk at least 1 km without pausing with Neurotropin®. If he failed to take Neurotropin®, he suffered from pain of the right lower limb. Four months later, he weighed 71.0 kg. He discontinued Neurotropin®, however, he did not feel pain during walking.
In the patient, weight reduction eliminated intermittent claudication without effective medicine. It is unclear whether the patient suffered from lumbar canal stenosis (LCS). Weight reduction is one of the first-line treatments in obese or overweight patients with LCS. Weight reduction is a safe and inexpensive treatment. Even if weight reduction does not alleviate symptoms, it improves overall health in former obese or overweight persons. However, we should not recommend weight reduction to patients whose first priority is maintaining of the amount of food.
Keywords: Lumbar canal stenosis; Intermittent claudication; Weight reduction; Overweight; Obesity; Neurotropin®
Introduction
Lumbar canal stenosis (LCS) is caused by narrowing of the spinal canal for some reasons at the lumbar level. Main symptom of LCS is intermittent claudication due to pain and/or numbness of the lower limb(s). Treatment of LCS is pharmacological therapy such as prostaglandin E1, epidural block, nerve root block, physical therapy, and operation, etc.
It is the basis of good health to maintain normal weight. Weight reduction is useful in patients with overweight or obesity. I report an overweight patent with intermittent claudication who responded to weight reduction.
Case Presentation
On January 6, 2018, a 58-year-old male visited Hiroshima Clinic because of intermittent claudication. He did not have a history of steroid use. He did not have skin abnormality of the lower back and buttocks. He did not undergo blood tests. In March 2014, he experienced intermittent claudication for the first time. In August 2015, he underwent a surgery for varicose veins of the both lower limbs. Intermittent claudication gradually worsened. In December 2017, he consulted a vascular surgeon, and there was no abnormality in the vascular system of the both lower limbs. At the initial visit, walking 10-100 meters caused pain in lateral part of the right lower limb, resulting in inability to walk. He was 162.1 cm tall and weighed 76.8 kg (body was index: 29.2). Pulse of both dorsalis pedis arteries was palpable. X-ray showed spina bifida occulta of the fifth lumbar vertebra and mild forward slip of the fifth lumbar vertebra (Figure 1). However, it was not clear whether the vertebral arch of the fifth lumbar vertebra had separation. On the same day, MRI did not show narrowing of the lumbar canal (Figure 2).
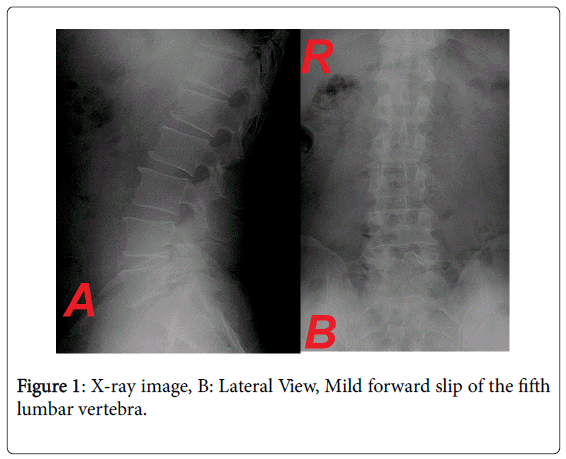
Figure 1: X-ray image, B: Lateral View, Mild forward slip of the fifth lumbar vertebra.
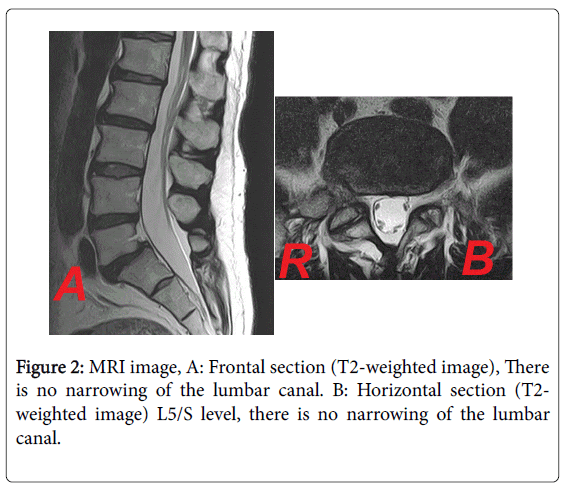
Figure 2: MRI image, A: Frontal section (T2-weighted image), There is no narrowing of the lumbar canal. B: Horizontal section (T2- weighted image) L5/S level, there is no narrowing of the lumbar canal.
I could not diagnose him as having LCS due to lumbar spondylolisthesis. Because he suffered from intermittent claudication due to pain of the right lower limb, there was the possibility. It is true that the fifth lumbar vertebra slipped forward, therefore weight reduction was recommended to prevent further slip. Eight tablets per day Neurotropin® were administered.
On February 3, 2018, he weighed 73.8 kg. He could walk at least 1 km without pausing. Four tablets per day Neurotropin® were administered.
On March 10, he weighed 73.6 kg. He did not feel pain of the right lower limb during one-day mountain climbing. If he failed to take Neurotropin®, he suffered from pain of the right lower limb
On April 14, he weighed 72.7 kg. From April 21, he started stretching exercise. From around May 5, he discontinued Neurotropin®, however, he did not feel pain during walking.
On May 19, he weighed 71.0 kg. He plans to gradually reduce body weight with a goal of body mass index 22 (58 kg) to prevent further slip.
Discussion
Pharmacological treatment often alleviates pain, resulting in reduce motivation of weight reduction. I am afraid that effective pharmacological treatment of pain may be harmful on this point. I explained as follows: Effective pharmacological treatment may be harmful because it may reduce motivation of weight reduction and weight reduction is necessary [1].
In the patient, weight reduction eliminated intermittent claudication without effective medicine. It is unclear whether the patient suffered from LCS. It is possible that weight reduction caused reduction epidural adipose tissue, eliminating intermittent claudication. However, strictly speaking, the reason why weight reduction eliminated intermittent claudication was unclear. It was reported that weight reduction improved symptom in obese patients with symptomatic lumbar epidural lipomatosis [2]. I think that the patient did not suffer from symptomatic lumbar epidural lipomatosis.
Weight reduction should not be underestimated. Weight reduction is one of the first-line treatments in obese or overweight patients with LCS (or intermittent claudication), regardless of whether the patients suffer from lumbar epidural lipomatosis or not. First, weight reduction is a safe and inexpensive treatment. If the amount of food is decreased, expenditures are rather reduced. Second, even if weight reduction does not alleviate symptoms, it improves overall health in former obese or overweight persons. Third, weight reduction probably decreases the progress of slipping of the lumbar spine in patients with slipping of the lumbar spine, regardless of whether the patients currently suffer from symptomatic lumbar spondylolisthesis or not.
Weight reduction is achieved with an increase of exercise quantity and/or decrease of amount of food. It is difficult for patients with intermittent claudication to walk over a long distance because of pain and/or numbness of the lower limb(s). It is very important in obese or overweight patients with (suspected) LCS. I recommend the following items. First, weight reduction should be less than 1.5 kg per month in patients whose weight is less than 80 kg. Second, body weight should be measured every day under identical conditions. If possible, a table of weight changes is made. Third, after supper, it should be avoided to take calories before the next breakfast. Forth, it is important to avoid the artificial sweetener aspartame. The details will be described later. Because it is very difficult to avoid all artificial sweeteners, I recommend avoiding aspartame alone. Fifth, alcoholic drinks and soft drinks are included in calories intake.
It is necessary to ask patients the first priority. Is maintaining of the amount of food the first priority? Is alleviation of symptoms the first priority? We should not recommend weight reduction to patient whose first priority is maintaining of the amount of food. Some patients whose first priority is maintaining of the amount of food answer “My first priority is alleviation of symptoms.” The excuses are as follows: “The amount of food is small.” “I do not have a breakfast.” “If body weight is decreased, nutritional status may be worsened.” Body weight is not decreased in such patients. In that case, I do not recommend weight reduction again. Individuals should take responsibility for individuals’ life.
As mentioned above, weight reduction is achieved with an increase of exercise quantity and/or decrease of amount of food. Weight reduction has some disadvantages. First, the greatest disadvantage of decrease of amount of food is to go against desire of appetite. It decreases the enjoy of life that persons eat as much as they want to eat. Second, drastic weight reduction is starvation itself and harmful to health. Drastic weight reduction is more likely to be weight rebound. As mentioned above, weight reduction should be less than 1.5 kg per month in patients whose weight is less than 80 kg. Third, some patients take the artificial sweetener aspartame. Suez et al. demonstrated that consumption of commonly used non-caloric artificial sweeteners formulations including aspartame drived the development of glucose intolerance through induction of compositional and functional alterations to the intestinal microbiota [3]. Although it is true that aspartame decreases calorie intake, there is no data that aspartame decreases body weight. Aspartame caused weight gain in mice [4]. I am afraid that persons who would like to reduce body weight should not take aspartame. Fourth, the core of increase of exercise quantity is walking. However, obese or overweight patients are more likely to suffer from osteoarthritis of the knee. Increase of exercise quantity often aggravates pain due to osteoarthritis of the knee. In case that exercise quantity is increased in such patients, walking in water or exercise in a sitting position is recommended.
Conclusion
An overweight male patient suffered from intermittent claudication due to pain of the right lower limb. X-ray showed mild forward slip of the fifth lumbar vertebra. MRI did not show narrowing of the lumbar canal. Neurotropin® eliminated intermittent claudication. If he failed to take Neurotropin®, he suffered from pain of the right lower limb. Weight reduction of approximately 6 kg eliminated intermittent claudication without Neurotropin®. Weight reduction is one of the firstline treatments in obese or overweight patients with (suspected) LCS (or intermittent claudication).
References
- Toda K (2018) Is pharmacological treatment of pain harmful or beneficial? J Clin Invest Stud 1: 1-1.
- Borstlap AC, van Rooij WJ, Sluzewski M, Leyten AC, Beute G (1995) Reversibility of lumbar epidural lipomatosis in obese patients after weight-reduction diet. Neuroradiology 37: 670-673.
- Suez J, Korem T, Zeevi D, Zilberman-Schapira G, Thaiss CA, et al. (2014) Artificial sweeteners induce glucose intolerance by altering the gut microbiota. Nature 514: 181-186.
- Gul SS, Hamilton AR, Munoz AR, Phupitakphol T, Liu W, et al. (2017) Inhibition of the gut enzyme intestinal alkaline phosphatase may explain how aspartame promotes glucose intolerance and obesity in mice. Appl Physiol Nutr Metab 42: 77-83.
Citation: Toda K (2018) A Case Whose Intermittent Claudication Disappeared After Weight Reduction. J Nov Physiother 8: 394. DOI: 10.4172/2165-7025.1000394
Copyright: © 2018 Toda K. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Share This Article
Recommended Journals
Open Access Journals
Article Tools
Article Usage
- Total views: 4722
- [From(publication date): 0-2018 - Mar 31, 2025]
- Breakdown by view type
- HTML page views: 3920
- PDF downloads: 802